


Welcome back to Ready, Set, Retina; in this episode, Daniel Epshtein, OD, FAAO, sits down with Carolyn Majcher, OD, FAAO, to discuss how to identify an inherited retinal disease (IRD) on ophthalmic imaging as well as diagnostic and management pearls.
Inherited retinal disease case report
Dr. Majcher began by introducing a case study in which a 15-year-old Native American female was referred to her clinic for worsening blur at distance with new glasses from 6 months ago. The previous optometrist performed a macular optical coherence tomography (OCT) and discovered abnormalities, which led them to refer the patient for further evaluation.
The patient had a past ocular history of vision therapy (VT) for accommodative spasm and a previous diagnosis of Streff syndrome. Additionally, her medical history and family history were unremarkable for contributing factors, and her entrance testing and external exam were normal. Her tonometry was 14/14mmHg.
The patient reported a gradual reduction in vision over the course of several years, and her best-corrected visual acuity (BCVA) history was as follows:
- 2016: 20/25 OD/OS
- 2019: OD 20/70, OS 20/50
- 2020: 20/70 OD/OS
- 2022:
- OD -1.50-0.50x180 20/150 pinhole no improvement (PNHI)
- OS -1.75-0.50x180 20/150 PNHI
Using multimodal imaging to identify the IRD
Dr. Majcher ordered color fundus photography (seen in Figure 1), which revealed macular foveal mottling in a classic “beaten bronze” appearance that is typically seen in patients with Stargardt disease.
Additionally, there were yellowish pisciform flecks—sometimes called fundus flavimaculatus—which often accompany Stargardt disease as well. The funduscopic exam indicated the presence of bilateral symmetric retinal disease in a young patient; which is often consistent with an IRD.
Figure 1 is color fundus photography OU, highlighting a bilateral and symmetrical disease with a beaten bronze appearance and fundus flavimaculatus, which are clinical findings often seen in patients with Stargardt disease.

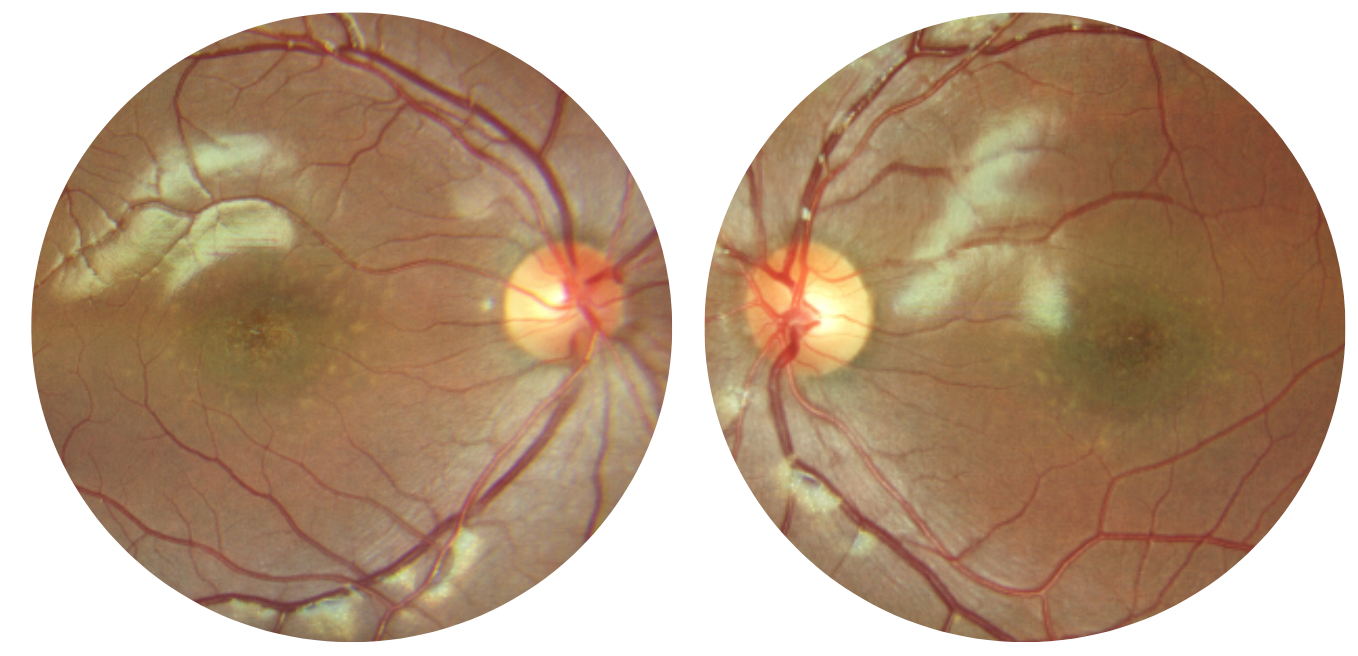
Figure 1: Courtesy of Carolyn Majcher, OD, FAAO.
Subsequently, Dr. Majcher performed fundus autofluorescence (FAF), which she finds particularly useful in outer retinal disease (especially in IRDs) because it allows for visualization of the full pattern of outer retina and retinal pigment epithelium (RPE) degeneration.
Yet again, the imaging showed bilateral symmetric patterns in FAF abnormalities. Centrally, there was hypoautofluorescence, suggestive of loss of the outer retina and RPE. This area of hypoautofluorescence was surrounded by a halo of hyperautofluroescence, which is indicative of degenerating or sick retinal and RPE tissue.
Figure 2 demonstrates FAF imaging with a central area of hypoautofluorescence encompassed by an area of hyperautofluorescence.

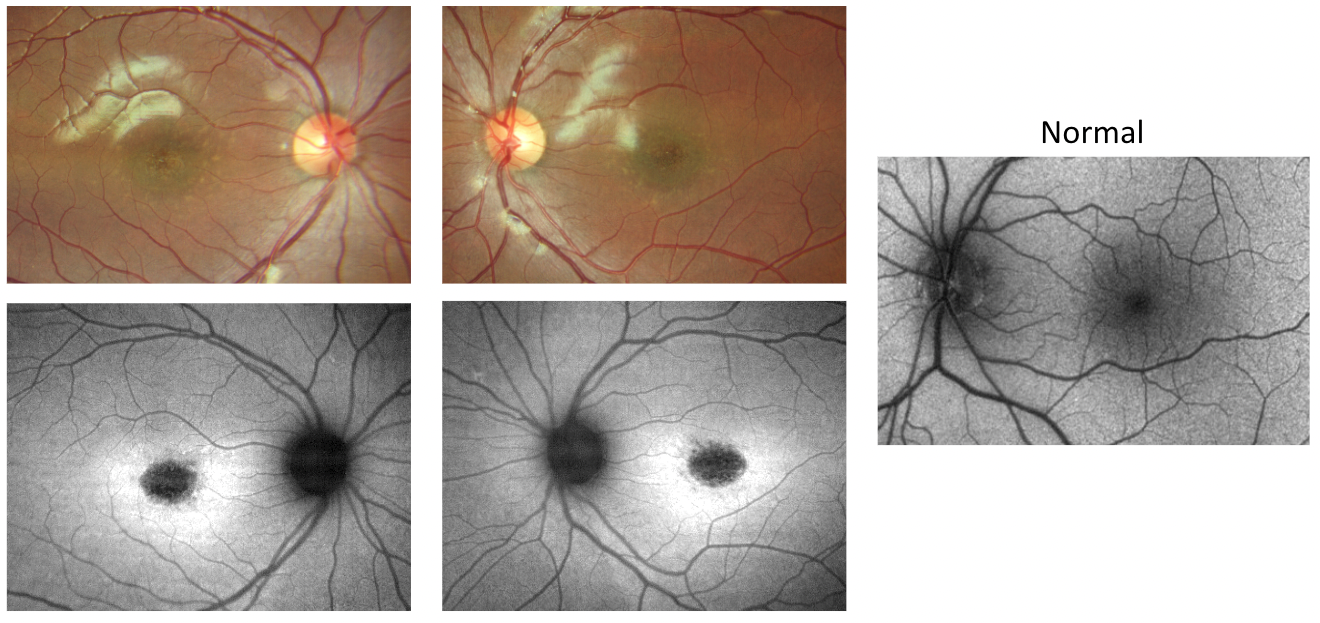
Figure 2: Courtesy of Carolyn Majcher, OD, FAAO.
Finally, the patient’s OCT imaging showed symmetric foveal outer retinal atrophy that was so severe almost all of the retina had atrophied in the center of both eyes. This, paired with the outer retinal atrophy, RPE atrophy, and the increased choroidal signal underlying the central atrophied retina, made an IRD high on the list of differential diagnoses.
Figure 3 highlights OCT imaging with severe central retinal atrophy and increased choroidal signal underneath.

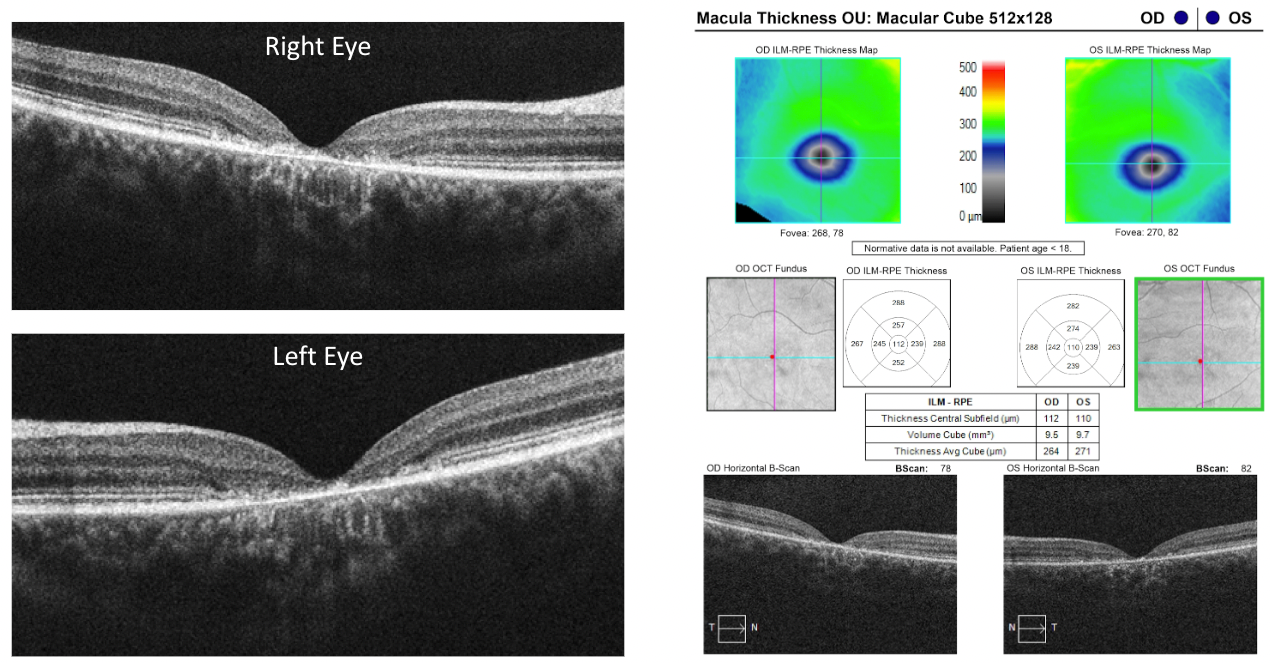
Figure 3: Courtesy of Carolyn Majcher, OD, FAAO.
IRD case report conclusion
The patient was referred to a retina specialist for genetic testing, which uncovered that the patient was homozygous for a retinol dehydrogenase 12 (RDH12) mutation, which is consistent with autosomal recessive Leber’s congenital amaurosis (LCA).
There are no genetic therapies for this inherited condition at this time unless the genetic mutation is RPE65, in which case Luxturna is available. Consequently, the patient was referred for low vision and rehabilitative services.
The diagnostic approach for IRDs
When treating a patient suspected of having an IRD, Dr. Epshtein emphasized that he uses a step-wise approach to diagnose them by:
- Matching the patient’s clinical presentation to a known IRD.
- Using multimodal imaging, such as fundoscopic examination, OCT, and FAF, to identify symmetrical patterns of disease and retinal abnormalities.
- Ordering a genetic test and potentially referring the patient to a retinal specialist if appropriate.
Interestingly, in this case report, the clinical pattern more closely resembled Stargardt disease than LCA—specifically because the patient did not experience significant vision loss until later on in life. Whereas in most phenotypes of LCA, the vision loss is severe within the first year of life.
This highlights how there can be significant variability between genotype and phenotype in IRDs. Case in point, although the patient has LCA, she didn’t automatically qualify for Luxturna because her genetic mutation was not RPE65.
Additional diagnostic testing for IRD patients
Electrodiagnostic testing
Dr. Majcher reaffirmed that OCT and FAF are invaluable for examining patients to determine if they have an IRD. Occasionally, she also uses electrodiagnostic testing such as electroretinography (ERG)—a non-invasive, functional test that can detect objective retinal function—in IRD patients.1
To elucidate when she uses electrodiagnostic testing, she outlined two potential situations:
- If genetic testing comes back positive for a specific mutation that matches the clinical scenario, wherein the diagnosis can be made, and the patient counseled on how to manage the condition.
- If a genetic test comes back positive for a mutation of unknown significance or if it is unclear whether the genetic mutation is directly causing the clinical presentation, electrodiagnostic testing can be helpful in determining the source of the retinal dysfunction.
Genetic testing
Genetic testing can help eyecare practitioners (ECPs) rule out differential diagnoses between IRDs, and it provides information that can be used to counsel the patient, such as outlining the chance that their children could get the disease and the visual prognosis.
Further, knowing the exact genetic mutation allows ECPs to offer motivated patients the chance to enroll in clinical trials. Additionally, Dr. Epshtein noted that there are sponsored free programs that ECPs can take advantage of to get more information and access to genetic testing.
Conclusion
In summary, the diagnostic approach for IRD patients includes matching the patient’s clinical presentation to one of an IRD, evaluating the patient with fundoscopic, OCT, and FAF imaging to check for retinal abnormalities, and, if appropriate, ordering a genetic test.
Depending on the results of the genetic test, electrodiagnostic testing can be recommended to determine the source of retinal dysfunction.
As genetic testing becomes increasingly accessible to ECPs and patients via open-access databases, such as the My Retina Tracker Registry from the Foundation Fighting Blindness,2 it is imperative that ECPs remain aware of emerging genetic technologies and treatments to advance patient care.


