
SMILE, or Small Incision Lenticule Extraction, is the newest option in refractive surgery. Since first becoming available outside the U.S. in 2010, SMILE has quickly gained recognition as a revolutionary treatment that is transforming laser eye surgery into a minimally invasive, key-hole procedure. SMILE differs from other laser eye treatments in that it only requires a small laser incision to remove the target tissue and correct the vision. The treatment revolves around the incredibly precise VisuMax femtosecond laser (Carl Zeiss Meditec Inc, Jena, Germany) which can create an extremely precise stromal lenticule (below). To date, more than 1.5 million procedures have been performed by more than 1000 surgeons across the globe.

Intraoperative OCT B-scan taken during SMILE. The full stromal lenticule can be seen immediately prior to removal.
SMILE, even in its relative infancy compared to LASIK, has been shown to provide great results with more than 95% of patients achieving 20/20 uncorrected distance visual acuity.1 The U.S. FDA trial data also showed encouraging results with 88% of patient achieving 20/20 uncorrected distance visual acuity.2 SMILE was initially approved to treat spherical myopia up to -10.00 D in the U.S. so patient selection had to be tailored accordingly. In early October the FDA updated the approval to include astigmatism up to 3 D, which will open up this treatment option to a much broader range of your patients.
It is important to remember that SMILE is not better or worse than LASIK or PRK. Each procedure may offer benefits, but this must be evaluated on a patient by patient basis rather than to generalize as a whole. We have been performing SMILE, here in London, since 2012 and have fantastic outcomes. In our clinic all 3 procedures are charged at the same fee and are spoken about on an equal level when discussing options with the patient. With that being said, there will always be a reason why one procedure is chosen over another for any particular patient. In some cases, when the patient is a candidate for both, SMILE can offer a few benefits over LASIK. SMILE provides faster dry eye recovery, may leave the cornea with more strength, and patients can return to contact sports and activities the next day.3-5
Finally there are a few things to remember when it comes to co-managing a SMILE patient. The first is that candidacy for SMILE is essentially the same as it is for LASIK. A full corneal refractive surgery evaluation is performed, just as with any other laser patient. Patients should have unremarkable ocular and corneal health including normal topography, tomography, and epithelial measurements.
Postoperatively there may be a slight difference in healing so it is important to educate the patient before surgery. SMILE has a slightly longer healing time compared to LASIK, with most patients reaching their best uncorrected visual acuity 5-7 days after surgery compared to 1-2 days with LASIK. This difference in recovery time will continue to shrink because the recent FDA approval, along with expanding the treatment parameters to include astigmatism, included an extended range of laser settings which includes energy levels and other more complex changes. These settings are the key component improving visual recovery. Thus, you should expect your future SMILE patients to reach their maximum visual potential more quickly than before. In our clinic, 80-90% of patients are 20/20 the day after treatment.
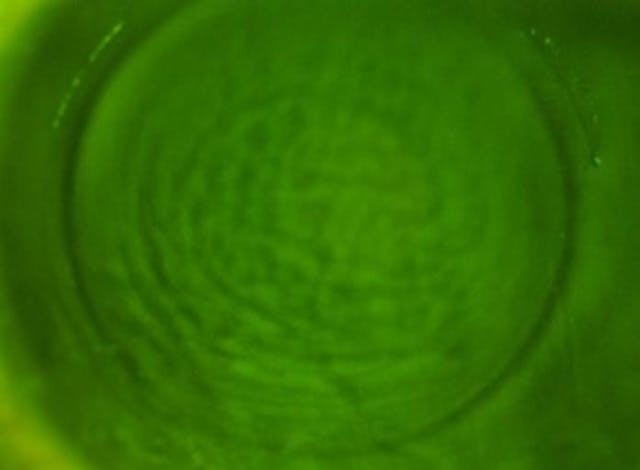
The second thing to take notice of is the presence of any cap wrinkles during the early postoperative period. These are best seen using heavy fluorescein staining at the slit-lamp (below). Even very small changes can delay visual recovery and should be sent back to the surgeon to smooth out.


Mild concentric cap wrinkles highlight with fluorescein dye immediately following treatment.
Finally, as with LASIK, it is important to make sure there is no inflammatory reaction the day after surgery. In LASIK, keratitis appears as a diffuse scattering of white cells in the flap interface.6 In SMILE, there can be a unique appearing keratitis that can present as very small focal infiltrates.7 These cases should be managed with aggressive steroids and referred back to the treating surgeon.
The introduction of SMILE to treat myopia and astigmatism adds another great option to offer to patients who wish to pursue surgical vision correction.
References
- Pradhan KR, Reinstein DZ, Carp GI, Archer TJ, Gobbe M, Dhungana P. Quality control outcomes analysis of small-incision lenticule extraction for myopia by a novice surgeon at the first refractive surgery unit in Nepal during the first 2 years of operation. J Cataract Refract Surg. 2016; 42:267-274.
- FDA. VisuMax femtosecond laser system for refractive correction (PMA), 2016.
- Reinstein DZ, Archer TJ, Randleman JB. Mathematical Model to Compare the Relative Tensile Strength of the Cornea After PRK, LASIK, and Small Incision Lenticule Extraction. J Refract Surg. 2013; 29:454-460.
- Randleman JB, Dawson DG, Grossniklaus HE, McCarey BE, Edelhauser HF. Depth-dependent cohesive tensile strength in human donor corneas: implications for refractive surgery. J Refract Surg. 2008; 24:S85-89.
- Reinstein DZ, Archer TJ, Gobbe M, Bartoli E. Corneal sensitivity after small-incision lenticule extraction and laser in situ keratomileusis. J Cataract Refract Surg. 2015; 41:1580-1587.
- Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. J Cataract Refract Surg. 2000; 26:1072-1077.
- Stuart A, Reinstein DZ, Vida RS, Archer TJ, Carp G. Atypical presentation of diffuse lamellar keratitis after small-incision lenticule extraction: Sterile multifocal inflammatory keratitis. J Cataract Refract Surg. 2018; 44:774-779.

