


Accommodative esotropia (ET) is a common childhood strabismus that will be encountered by most optometrists. This binocular condition has been studied and recorded time and again in research and literature, which provides eyecare professionals with a vast array of available resources.
Optometrists will usually provide the first line of treatment in accommodative ET. Depending on the optimum optical treatment outcomes, an orthoptist and/or ophthalmologist will be approached to continue the treatment, in collaboration.
This article provides a comprehensive overview on how to approach accommodative ET as journey—it is not a one stop destination.
Narrowing it down to accommodative ET
Your clinical journey starts with an accurate diagnosis. Rule out non-refractive components of the strabismus to narrow in on accommodative esotropia.
Strabismus (or squint) is a misalignment of the eyes, where the light rays from an image do not focus on corresponding retinal or bi-foveal points resulting in phoria or tropia. With phoria, the tendency is for an eye to drift out of alignment under latent conditions, but maintain fusion during manifest conditions.
Tropia, a manifest misalignment of the eyes, is a bit more complicated.
Tropia can be:
- Congenital, occuring during infancy, or it can be juvenile.
- Idiopathic or due to a refractive error.
- Acquired, either when:
- phoria breaks down into a tropia if decompensated by fatigue or illness
OR due to:
- Mechanical restriction
- Paresis or paralysis
Now, we’re getting closer to a precise diagnosis. Esotropia (ET) is a manifest inward turning eye, causing the light rays of the image to fall on the nasal retina. To narrow it further, accommodative ET is a childhood inward turning of the eye, most associated with an uncorrected hyperopic refractive error of +1.50D or more. As accommodative effort is exerted to correct hyperopia, over-convergence results in an esotropia.1, 2
Figure 1, below, represents the above information.

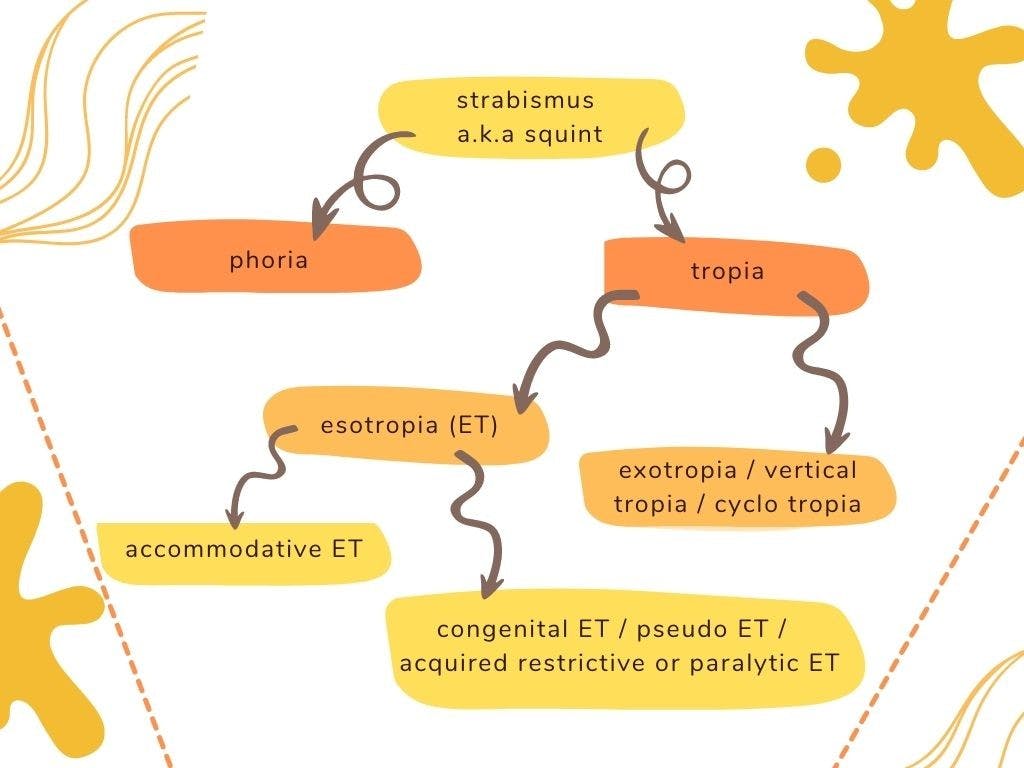
Figure 1: By author
To further aid in diagnosis, I have compiled a few key features of accommodative ET.
Key clinical features of accommodative ET1,2,3,4,5
- A positive family history of accommodative ET.
- Symptoms may include eye rubbing, squinting, headache, diplopia, and tired eyes.
- It is not congenital. The ET only manifests as the child learns to accommodate. Onset is between the ages of 6 months to 7 years, although it typically presents at about 2 years of age.
- The deviation angle is usually smaller than that of a congenital ET, commonly measuring 20-40ΔD.
- Initially accommodative ET may present as an intermittent ET when the child is looking at near, tired, or daydreaming. Ultimately, it may develop into a constant deviation.
- A hyperopic refractive error will be revealed by cycloplegic refraction, commonly of +1.50D to +6.50D.
Diagnosis
Use the flowchart below, in Figure 2, to assist with a more precise and timely diagnosis, which will ensure a better prognosis.
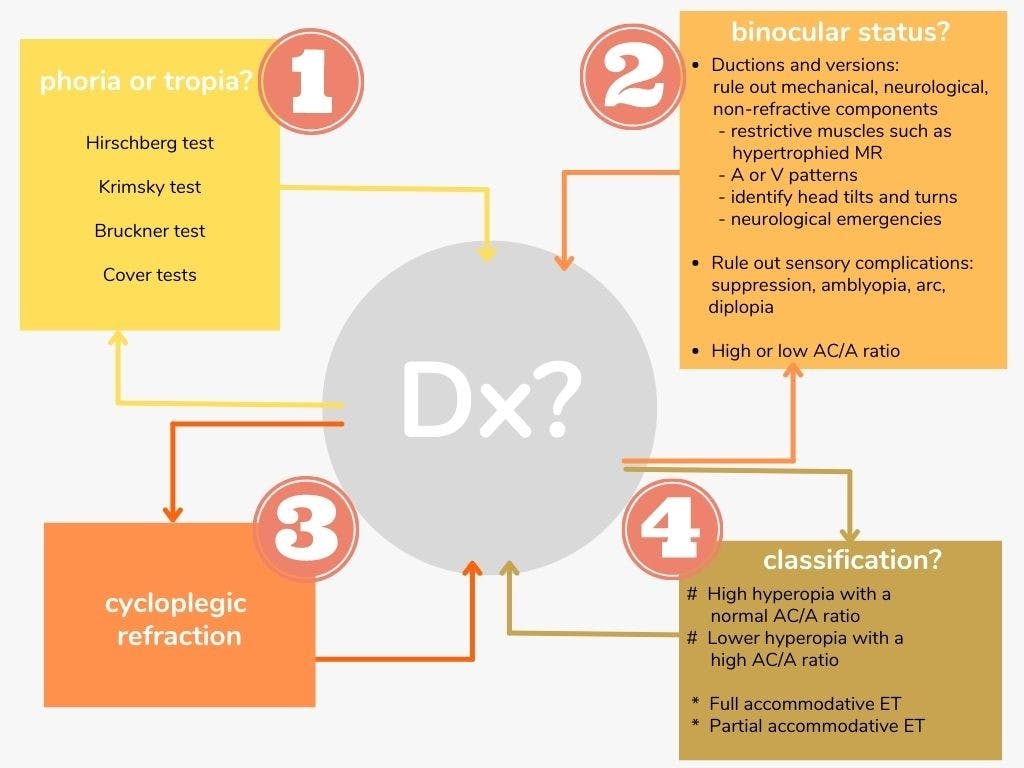
Figure 2: By Author
Cycloplegic refraction
Atropine 1% or cyclopentolate 1% can be used. Most modern-day optometry resources prefer cyclopentolate 1%, as the hyperopia revealed is clinically insignificant to that achieved by atropine, after 45-60min to administration. Darker irises usually require 1 to 2 drops more to be instilled, compared to a lighter-colored iris.1,5,6,7
Full cycloplegia through atropine 1% takes much longer, and the accompanying side effects like photophobia and blurry vision can last up to 10 days after use, which may interfere with school performance.1,6,7
Diagnostic pearls
The following key diagnostic facts can aid in guiding your diagnosis, as found relevant from my own practice and researched resources.
- Convergence can take place without accommodation, as it can be induced with BO prism, but accommodation is always accompanied by convergence.7
- Always perform a cycloplegic refraction on a pediatric patient suspected of an ET, as accommodative ET accounts for approximately half of childhood ET.4,7
- A poor correlation exists between maximum pupil dilation and full cycloplegia. A fully dilated pupil does not mean complete cycloplegia; verso full cycloplegia can be reached before maximum pupil dilation. Clearly the mydriatic effect lasts longer than the cycloplegia effect.1,8
- Accommodative ET with a high AC/A ratio are more common in children aged 2-3 years. The refractive error in this condition may be hyperopic, emmetropic, or even pseudomyopic. Therefore, a cycloplegic refraction is essential.6
- Associated findings and diagnosis include Brown’s syndrome, Duane’s syndrome, congenital nystagmus, and oblique over-actions.5
- Rule out latent vertical deviation components. The 30 min monocular patching technique can be used. Patch one eye for 30 minutes before evaluating ocular motility and alignment. This technique of dissociation will reveal latent deviations that could otherwise have been missed.9
Treatment options
After confirming your diagnosis of accommodative ET, you need to decide on the best suitable treatment for your pediatric patient.1,2,3,4
There are a range of different options outlined below:
(1) Optimum optical correction
Always give the full hyperopic cycloplegic prescription in infantile and juvenile accommodative ET. It is more important to obtain bi-foveal fixation and eliminate amblyopia in these critical age groups, than conserving and allowing for emmetropization development with under-correction of the hyperopia.1,2,3,4
The visual aid should do all the work to obtain clear vision, the eyes should relax. Parents need to understand that the eyes will still ‘cross’ when the spectacles are removed.
Single vision spectacles or contact lenses
A high index and/or an aspheric spectacle lens design will improve cosmesis, by reducing the magnified, ‘big-eyes’ look. The correct frame choice is important to fit well and be suitable for the increased convex shaped lens.
Bifocal spectacles or contact lenses
An infant’s world is mainly near-based, thus near fusion is essential, even if distance fusion is present.
When the full cycloplegic hyperopic prescription is in place, allowing for ortho-tropia at distance, but a residual esotropia of more than 10ΔD is measured with near fixation, a high AC/A ratio should be suspected. Bifocals should be prescribed to encourage fusion with near fixation. The add power should be strong enough to keep the near esophoria below 10ΔD, ideally +2.50D or +3.00D.1,2,3,4
Bifocals should be fitted on mid-pupil and a large segment width of 35mm is advised. Frames should not drop down the nose; a proper fit is required. Atropine 1% can be prescribed to encourage using the near segment if the child is not initially using the bifocal correctly.1,2,3,4
(2) Orthoptics
Orthoptic visual therapy should be part of the treatment plan when sensory complications are diagnosed. The treatment plan should aim for single, clear, comfortable, binocular vision, which means:3,4,10
- Eliminating amblyopia
- Overcoming suppression
- Encouraging fusion
- Stimulating fusional divergence3,4,10
(3) Surgical intervention
After optimum optical correction is prescribed (single vision or bifocal), and a residual esotropia of more than 10ΔD is still measured, a partial accommodative ET is present (not fully refractive).1-3
This warrants a referral to an pediatric ophthalmologist specializing in strabismus surgery. Surgical intervention may be required to achieve fusion. Treatment should not be delayed.1-3
Refractive laser surgery
As full accommodative ET is refractive in nature, refractive laser surgery may play an integral part in the management thereof. It may reduce the need for strabismus surgery and limit amblyopia with timely intervention. Though there are some controversies between ophthalmological opinions regarding this treatment approach, it would mean careful patient selection, justified on a case-by-case basis.9,11
The best candidates would obviously be those with good fusion, stereopsis, and ocular motility. No latent vertical deviations should be present. Other candidates will include those not coping with initial treatment strategies or older children who did not outgrow their accommodative ET. 9,11
Careful consideration should be taken with post-operative diplopia, residual deviations, and residual astigmatism. The patient needs to understand that they may not be spectacle free or independent.9,11
(4) Pharmaceutical: Miotics
Miotics are not a common choice of treatment; thus, this article will not elaborate in depth. It may however be indicated in infants who do not cope with optical correction (spectacles/contact lenses). Careful consideration should be taken with this choice of treatment as toxic side effects can occur. Strict follow up routines should be practiced.1,3
Management plan and follow-up schedule
When you have decided on the best suitable treatment for your patient, a management protocol and follow-up routine should be agreed upon. Remember, there is no “one-size-fits-all”. Adjust the management plan according to your clinical observation and diagnosis, to yield the best possible prognosis. You can use the following guidelines.1,3,4,5
With a goal of alignment, fusion, stereopsis, keep in mind:
- Optical correction should be worn full time.
- The first follow-up visit should not be delayed after wearing and adapting to the initial optimum optical correction for 2 to 3 months. If a high distance or near ET is still measured with correction, a repeat cycloplegic refraction should be done to hunt for residual uncorrected hyperopia, and the optical correction should be adjusted accordingly. If there is no evidence of residual refractive components, the patient should be treated for partial accommodative ET. Also evaluate for sensory complications that need orthoptic intervention.
- A small residual esophoria of less than 10ΔD is favorable at near to encourage fusional divergence.
- Don’t forget to correct the underlying astigmatism for the best corrected vision.
- The next follow up visit can be after 6months to ensure a stable binocular status.
- Once stable outcomes are achieved, an annual follow-up schedule can be agreed upon. With these visits, it can be considered to reduce the hyperopic prescription with 0.75D steps, but it is essential to maintain fusion at distance and near fixation.1,3,4,5
Prognosis
Diagnostics, treatment, signs and symptoms will differ from patient to patient. It is important to emphasize realistic expectations concerning the prognosis.
Factors influencing prognosis include:
- Age of onset: Expect a worse prognosis with an earlier age of onset (e.g., younger than 2 years of age)
- Constant vs intermittent: A constant uncorrected ET is at higher risk of developing amblyopia, compared to an intermittent ET where fusion is variably stimulated
- Sensory complications: The presence of fusion, stereopsis, amblyopia, and suppression will affect the outcome
- Treatment delay: Earlier intervention improves prognosis
- Circumstances: Economic and social factors can contribute to delayed treatment, follow-up consultations, and up-to-date optical correction or surgery
- Improvement: Ss hyperopia and the AC/A ratio is expected to decrease after the age of 8 years, the ET should be reduced, Although 50% of patients show a persisting accommodative ET after 10 years of age.
- Full vs partial accommodative ET: Timely surgical intervention will be required with partial accommodative ET
- Surgical intervention: Subsequent surgery and post-operative optical correction might still be required1,3,4
Conclusion
Here are a few takeaways for the diagnosis and treatment of accommodative esotropia:
- Bust the myth: “My child is too young for spectacles!”
- Education, education, education! Patients and parents need to understand that accommodative ET is not a quick fix, although it can be treated and managed. Timely intervention is key. You and your patient need to adhere to a strict, follow-up schedule.
- Encourage parents and family members to be alert for acquired esotropia. Getting this message conveyed to other pediatric healthcare professionals can assist with prompt referrals.
- Each patient case should be addressed individually. All journeys do not travel the same routes, nor reach the same destination. Ensure the traveler is aware!
References
- K.W. Wright, P.H. Spiegel, L.S. Thompson. Handbook of Pediatric Strabismus and Amblyopia. New York : Springer Science+Business Media,Inc., 2006. pp. 243-254. ISBN 0-387-27924-5.
- Accommodative Esotropia. AAPOS. [Online] March 2019. https://aapos.org/glossary/accommodative-esotropia.
- Roy, F.H. Practical Management of Eye Problems: glaucoma, strabismus, visual fields. Philadelphia : Henry Kimpton Publishers, 1975. pp. 114-116. ISBN 0-8121-0501-X.
- J.A. Pratt-Johnson, G. Tillson. Management of Strabismus and Amblyopia. New York : Thieme, 2001. pp. 109-124. ISBN 0-86577-992-9.
- G.R. Diamond, H.M. Eggers. Strabismus and Pediatric Ophthalmology. London : Mosby, 1993. pp. Chap8.1-8.12. ISBN1-56375-011-2.
- Olitsky, S.E., Chan, E.W. and Farzavandi, S. Strabismus: Accommodative Esotropia. [Website article] s.l. : AAO, January 2016.
- Raab, Professor Dr Edward. Lecture: Accommodative Esotropia and its complications. [Webinar] New York : Cybersight, 2017.
- Time of maximum cycloplegia after instillation of cyclopentolate 1% in children with brown irises. S. Laojaroenwanit, V. Layanun, P. Praneeprachachon, P. Pukrushpan. [ed.] DovePress. Aukland, N.Z. : Clinical Ophthalmology, May 18, 2016, Vol. 10, pp. 897-902.
- Rainey, A.M. What you should know before you perform LASIK on a strabismus (or any) patient. [Website article] Houston : CRSToday, March 2003.
- Orthoptic Managment of Accommodative Esotropia. Moore, S. and Cohen, R.L. 1, 1977, American Orthoptic Journal, Vol. 27, pp. 119-123.
- Astle, W.F. and Huang, P.T. Another perspective on Pediatric laser refractive surgery. [Online] July/August 2010. https://crstodayeurope.com/wp-content/themes/crste/assets/downloads/0710CRSTEuro_refsurg.pdf.


