



What if you could halt the progression of a lifelong disease with a single treatment? Circumvent slow visual debilitation, major eye surgery, and years of careful postoperative care? This is the hope that corneal cross-linking (CXL) gives to patients with corneal ectasia, and the reason why this new technology has become a major hot topic in the field of corneal disease.
Indications for cross-linking
CXL is used to treat corneal ectasia, a group of disorders associated with weakening, thinning, and distension of the corneal shape. Two major indications include keratoconus and post-refractive ectasia.
Keratoconus
Keratoconus is characterized by progressive cone shaped deformation of the cornea, with an estimated prevalence of 1 in 2000 people. Its pathogenesis is multifactorial; keratoconus is associated with over 60 genes, various systemic disorders, eye rubbing, and atopy, all of which culminate in Bowman’s membrane disruption, weakening and thinning of the corneal stroma, and conical protrusion of the cornea.
The disease typically begins in adolescence and progresses into adulthood prior to stabilizing. Patients present with rapidly increasing myopia and high irregular astigmatism. Topography/tomography show inferior steepening with high keratometric values (Ks), against-the-rule astigmatism, and thinning greatest at the corneal apex. Severe cases may develop tears in Descemet’s membrane known as corneal hydrops, resulting in acute pain and corneal edema.
Patients with keratoconus lose vision due to increasing refractive error, higher order aberrations, and in late stages, corneal scarring. As the disease progresses, patients move from prescription lenses to rigid gas permeable (RGP) contacts to contact lens intolerance. In advanced cases, the only recourse is a corneal transplant such as deep anterior lamellar keratoplasty (DALK) or penetrating keratoplasty (PKP). Like any other transplant, patients face months of visual rehabilitation, years of steroid eye drops to prevent rejection, and the risk for organ failure necessitating repeat transplantation.
Ectasia after refractive surgery
Corneal ectasia is a rare but vision-threatening complication of refractive surgery, and has been reported after laser in situ keratomileusis (LASIK), photorefractive keratectomy (PRK), and small incision lenticule extraction (SMILE). Risk factors for ectasia include thin corneas, low residual stromal bed thickness, high corrections, and predisposing conditions such as forme fruste keratoconus.
Similar to keratoconus, patients with post-refractive ectasia develop worsening vision from progressive myopia, irregular astigmatism, corneal steepening, and corneal thinning. Treatments include refractive correction, RGPs, and corneal transplantation.
Criteria for cross-linking
In 2016, the United States Food and Drug Administration (FDA) approved the Avedro corneal CXL system for the stabilization of progressive keratoconus and post-refractive ectasia. Patient criteria were largely derived from keratoconus trials, although these are easily applied to post-refractive ectasia.
Good candidates for CXL include patients with mild to moderate disease demonstrating Kmax > 47.0, inferior-to-superior K ratio > 1.5, corneal thickness after deepithelialization > 400 um, best corrected visual acuity (BCVA) < 20/20, and evidence of disease progression. There is no global consensuson specific criteria for progression, and criteria vary from study to study. Common definitions of progression include an increase in Kmax > 1.0 D, Kmean > 0.75 D, or cylinder > 1.0; or a decrease in spherical equivalent > 0.5 D or CCT > 2% over 12 months (Table 1).
Table 1. Guideline of indications for corneal cross-linking. K: keratometric value, D: diopter. IS ratio: inferior-to-superior ratio, CCT: central corneal thickness, BCVA: best corrected visual acuity, HSV: herpes simplex virus. Values may vary across studies.

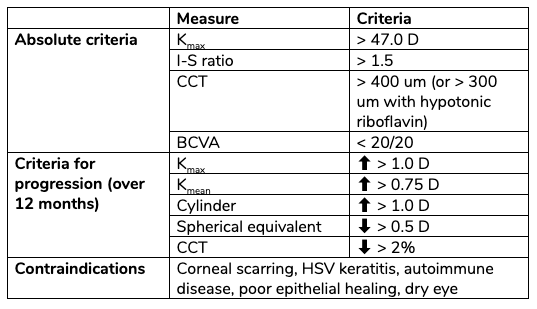
Contraindications for CXL include advanced ectasia with corneal scarring, history of herpes simplex virus (HSV) keratitis, autoimmune disease, risk factors for poor epithelial healing, and dry eye.
Cross-linking protocols
CXL utilizes a photochemical reaction to form covalent bonds (cross-linkages) between collagen molecules in the corneal stroma, strengthening the cornea to prevent further deformation. The cornea is treated with riboflavin (vitamin B2), then exposed to ultraviolet-A (UVA) light. Upon UVA absorption, riboflavin molecules reach an excited state and produce free radicals, which in turn induce collagen polymerization without altering corneal transparency. The different protocols for CXL are summarized in Table 2.

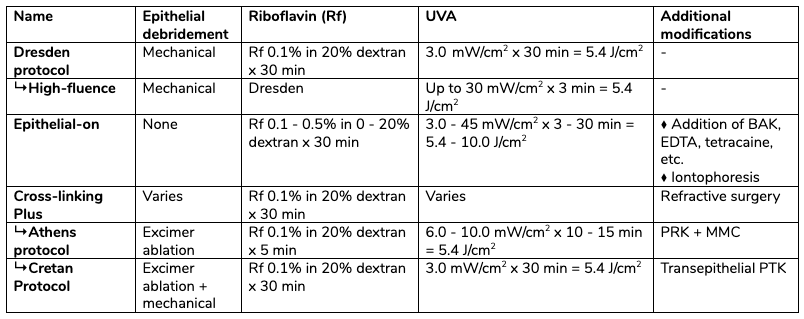
Table 2. Summary of corneal cross-linking protocols. UVA: ultraviolet light-A. BAK: benzalkonium chloride. EDTA: ethylenediaminetetraacetic acid. PRK: photorefractive keratectomy. MMC: mitomycin-C. PTK: phototherapeutic keratectomy.
Dresden protocol
Spoerl and Wollensak at the University of Dresden first described CXL for corneal ectasia in 1998, then its use in keratoconus in 2003. The original protocol instructs removal of the central 8.0 – 9.0 mm of corneal epithelium, then application of riboflavin 0.1% with 20% dextran for up to 30 minutes, followed by UVA 365 – 370 nm irradiation at 3.0 mW/cm2 for an additional 30 minutes, for a total energy of 5.4 J/cm2. CXL should be performed on corneas with a minimum of 400 um thickness to avoid endothelial damage, although hypoosmolar riboflavin may be used to hydrate thinner corneas to achieve > 400 um thickness prior to UVA application.
Theoretically, alternate combinations of illumination intensity and duration can produce an equivalent treatment in terms of total energy applied, although this relationship may not translate linearly to clinical practice. Accelerated high-fluence protocols using irradiance of up to 30 mW/cm2, with total energy maintained at 5.4 J/cm2, show similar efficacy, though further study is needed.
Epithelium-on cross-linking
By forgoing epithelial debridement, epithelium-on CXL offers decreased pain, faster recovery, and lower risk for serious complications such as infectious keratitis, endothelial damage, and stromal melt compared to traditional epithelium-off techniques. However, the corneal epithelium is a barrier to both riboflavin and UVA penetration, which may reduce treatment efficacy.
Various modifications have been described to enhance delivery of riboflavin and UVA to the corneal stroma. Adjunctive agents such as benzalkonium chloride, tetracaine, ethylenediaminetetraacetic acid (EDTA), gentamicin, or trometamol mixed into the riboflavin solution can loosen epithelial tight junctions. Increasing the riboflavin concentration up to 0.5% and decreasing or eliminating dextran can also promote riboflavin penetrance. High-fluence protocols, including ones with increased total energy up to 10 J/cm2, enhance the depth of UVA penetration. Finally, iontophoresis-assisted epithelium-on CXL uses an electric current of 1 mA over 5 minutes to deliver negatively charged riboflavin molecules across the corneal epithelium.
There are 3 epithelium-on CXL systems currently undergoing clinical trials: Ribostat (CXL Ophthalmics LLC), Ribocross TE (IROS SrL) with vitamin E solution (VE-TPGS), and Avedro with a new preparation of riboflavin (Paracel) with supplemental oxygen. Early results show promise, although further study is required to establish safety and efficacy.
Cross-linking with refractive surgery
While CXL may improve vision through its flattening effect, the primary outcome is to halt disease progression rather than eliminate refractive error. As such, studies have investigated whether CXL Plus, referring to CXL in conjunction with refractive procedures, can produce superior visual outcomes.
The Athens protocol entails epithelial debridement of 50 um with an excimer laser, then partial topography-guided stromal ablation to a maximum depth of 80 um, followed by high-fluence CXL using UVA 10 mW/cm2 for 10 minutes. Given the inherent corneal flattening with CXL, care should be taken during laser ablation to avoid overcorrection. The Athens protocol is effective for patients with mild to moderate disease with 350 – 450 um of corneal thickness and significantly improves uncorrected distance visual acuity (UDVA). However, results are widely variable and not necessarily superior to epithelium-off cross-linking alone.
In contrast to simultaneous combination therapy, sequential CXL followed by PRK 6 to 12 months later raises several concerns, including the unpredictable ablation rates of cross-linked corneas, further corneal thinning, and increased haze formation. Use of mitomycin-C (MMC) during CXL Plus is under debate, as CXL already clears anterior stromal keratocytes. If used, MMC is applied at a concentration of 0.02% for 20-30 seconds during PRK.
The Cretan protocol describes transepithelial phototherapeutic keratectomy (PTK) with excimer laser ablation of 50 um of corneal epithelium in a central 6.5 – 7.0 mm zone, mechanical epithelial debridement to 8.0 – 9.0 mm, and finally conventional epithelium-off CXL. PTK allows precise removal of an irregular and diseased Bowman’s layer as well as smoothening of the anterior corneal stroma. Early studies of this technique boast better visual and safety outcomes, although further study is required.
Post-operative recovery and outcomes
After treatment, patients experience gradual visual recovery. Visual acuity and Ks often worsen in the first month, followed by improvement over 6 to 12 months as the corneal haze clears and epithelium remodels.
Complications
The most common complication after CXL is corneal haze. Distinct from post-PRK haze, post-CXL corneal haze presents as a dust-like appearance in the anterior stroma, which can increase in the first 1 to 3 months post-operatively but usually resolves over 6 to 12 months. A small subset of patients experience persistent, vision-limiting haze. Risk factors for corneal haze include thin corneas, high Ks, older age, insufficient riboflavin, and UVA overexposure.
While corneal flattening often improves vision, excessive flattening can threaten it; pediatric corneas are at highest risk for excessive flattening compared to adult populations. Corneal endothelial damage may result from direct damage by UVA in a cornea with inadequate thickness or from post-operative inflammation. Peripheral sterile ring-shaped infiltrates may occur and resolve with topical steroids. Although rare, other serious complications include infectious keratitis, persistent epithelial defect, and corneal melt.
Outcomes
The flagship feature of CXL is its ground-breaking ability to halt progression of corneal ectasia. In a 2017 randomized, double-blinded trial, patients who received epithelium-off CXL demonstrated a reduction in Kmax of 1.6 D, compared to a 1.0 D increase in the control group at 1 year. In addition, long-term studies have found that disease stability persisted through up to 10 years of follow-up. CXL prevents progression to advanced disease and obviates the need for corneal transplantation, improving its cost-effectiveness and patient quality of life.
The flattening effect with CXL has the added benefit of decreasing myopia. Patients report improved visual function across multiple measures, including photophobia, night driving, reading, diplopia, and glare. However, the 2017 trial found continued progression of corneal ectasia in 6% of patients, with other studies reporting treatment failure rates as high as 33%. Of note, corneal thickness can decrease after CXL due to compaction of stromal collagen fibers but does not necessarily indicate progression of ectasia.
There is mixed evidence regarding the efficacy of newer CXL protocols such as epithelium-on and CXL Plus, with some studies finding equivalent outcomes and others inferior compared to epithelium-off. As of now, epithelium-off CXL holds the gold standard in terms of clinical efficacy. Further study with randomized controlled trials and long-term follow-up is required to determine the optimum protocol that maximizes efficacy while minimizing complications.
Take-home points
- Collagen cross-linking is approved by the FDA as a safe and effective method for the stabilization of keratoconus and post-refractive ectasia.
- The cornea is treated with riboflavin, then UVA, to induce covalent cross-linkages that strengthen the cornea.
- Epithelium-off cross-linking is more effective, but epithelium-on has fewer complications. Modifications to epithelium-on techniques to enhance efficacy are under study.
- Cross-linking can be combined with PRK to improve refractive error.
- Corneal haze is a common post-operative complication, but usually resolves over 6-12 months.


