



Behçet’s disease (BD) is a chronic, relapsing, inflammation-causing multisystemic vasculopathy with ocular and systemic manifestations. In 2019, apremilast was approved for managing oral ulcers associated with BD. To our knowledge, no studies have reported the efficacy of apremilast in managing recurrent uveitis in BD. In this article, we describe a case with recurrent unilateral uveitis associated with BD that was successfully managed by apremilast.
Case background
BD is a multisystemic vasculopathy of unknown etiology causing ocular and systemic manifestations. BD results from autoinflammatory dysregulation of macrophages and CD4 T-cells associated with mutations in HLA-B*57. BD is characterized by findings such as oral or genital ulcers, eye lesions, and a positive pathergy test. Behçet’s uveitis (BU) presents with ocular manifestations involve non-granulomatous inflammation with or without occlusive vasculitis. BU could cause vision loss and blindness, and therefore prompt treatment is warranted.
Pathogenesis of Behçet’s disease
BD is associated with the class 1 antigen named HLA-B*51. HLA-B*51 mutations have been associated with increased activity of T-cells and mononuclear cells important in pathogenesis of BD. An HLA-B*51-restricted peptide has been shown to activate proliferation of peripheral blood mononuclear cells only seen in HLA-B*51-positive BD patients with posterior uveitis.7
Clinical Manifestations of Posterior Uveitis in Behçet’s disease
BU is defined as nongranulomatous panuveitis and retinal vasculitis. BD with posterior uveitis presents with typical signs of diffuse vitritis, sheathing of retinal veins, and occlusive vasculitis. A sudden onset of uveitis flares with spontaneous resolution is a diagnostic feature of BD. Diffuse vitritis is a constant feature of posterior uveitis, and vitreous haze usually most severe at the onset of attack indicates inflammatory activity. Breakdown of the blood-retinal barrier causes recurrent hemorrhages along inflamed retinal vessels and retinal vein occlusion.3
Most common complications of BU include cataract, posterior synechiae, macular edema, optic atrophy, and glaucoma. Rare but significant complications can occur, including retinal neovascularization, retinal tears, and detachment, hypotony, and phthisis bulbi. Permanent vision loss is most commonly a result of maculopathy and optic atrophy.3
Diagnosis of Behçet’s disease
BD can be diagnosed using the ICBD Criteria with any two of the following findings (oral apopthosis, genital apathosis, eye lesions, vascular lesions, or a positive pathergy test).8
Management of Uveitis in Behçet’s disease
Ocular inflammation in BD can be monitored clinically or with imaging. Anterior chamber cells, retinal infiltrates, and sheathing of retinal veins are signs of ocular inflammation but can be difficult to determine if an eye is completely quiet or not. Fluorescein angiography (FA) is the gold standard to monitor ocular inflammation in BD and severity of retinal ischemia. Posterior inflammation in BD manifests as leakage from retinal vessels on FA.3
Immunotherapy is the mainstay therapy for ocular manifestation in BD. Azathioprine, cyclosporine-A, interferon-α, infliximab, and monoclonal TNF-α antibodies, are used for BD involving the posterior segment of the eye.1,3 Systemic glucocorticoids are indicated as adjuncts to other systemic immunosuppressants.2 Corticosteroids with azathioprine and/or cyclosporine is first line therapy for posterior inflammation in BD. In resistant cases, biologic agents, such as interferon-α or infliximab, are used.3
Apremilast is an orally administered phosphodiesterase 4 inhibitor that prevents degradation of cyclic adenosine monophosphate, decreased production of tumor necrosis factor α, interleukin-2, interleukin-8, interleukin-12, interleukin-17, and attenuated response of inflammatory responses from Th1, Th17, and M1 macrophages.3,4 In 2019, apremilast was approved for managing oral ulcers associated with BD, showing no evidence of worsening uveitis or other adverse events in major organs in the treatment group, receiving apremilast 30 mg orally twice daily during a 28 week follow-up. Two patients, one with anterior uveitis and the other with panuveitis, in the placebo group had active uveitis flares during the placebo-controlled period.4 To our knowledge, no studies have reported the efficacy of apremilast in managing recurrent uveitis in BD. In this report, we describe a case with recurrent unilateral uveitis associated with BD that was successfully managed by apremilast.
Case report
A man in his mid-50s presented with increased floaters and blurry vision right eye (OD) for one week prior. He denied any eye pain. He had a known history of BD for which he was followed by rheumatology. The patient reported a concurrent history of genital and oral ulcers every 2-3 months for several years that had been treated with oral steroids and subtenon steroid injections in the past.
On examination, his best-corrected visual acuity was 20/40 OD and 20/20 left eye (OS). Intraocular pressure was normal for both eyes (OU). Anterior segment examination OU revealed no inflammation and mild nuclear sclerotic cataract OU. Posterior segment examination OD showed moderate vitreous debris and anterior vitreous cells. There were punctate dot blot hemorrhages in the mid peripheral retina inferotemporally OD. Posterior segment examination OS did not show any signs of inflammation. Optical coherence tomography (OCT) of the macula showed areas of retinal thinning without edema OU. Fluorescein angiography (FA) OD showed trace leakage at the vessels just distal to the inferotemporal arcade and mild blockage from the scattered hemorrhages.
The patient was started on oral prednisone 100 mg once daily. Oral prednisone was gradually tapered and used as a bridge for azathioprine. The patient was put on azathioprine 50 mg once daily initially, which was gradually increased to 150 mg once daily. The patient noted intolerable fatigue with this regimen over the course of approximately six months, and thus methotrexate was initiated at 7.5 mg once weekly, which was gradually increased to 20 mg once weekly. Due to the limited effect of methotrexate on his oral and genital ulcers for approximately one year, methotrexate was discontinued and oral apremilast was initiated. While on apremilast, the patient had no recurrences of ocular and systemic manifestations for BD for the past two years. His vitritis OD gradually dissipated over the initial one year of systemic anti-inflammatory therapy, and his vision improved to 20/20 OD.
Discussion
Currently, apremilast is FDA-approved for managing oral ulcers in BD effectively.4 We present a patient with unilateral recurrent uveitis associated with BD who was placed on apremilast and has attained remission for two years. Our case suggests a potential role of apremilast in managing BD with uveitis. Further studies are required to elucidate the efficacy of apremilast in treating ocular manifestations related to BD.
Uveitis is reported in about 50% of cases of BD.1 Methotrexate and periocular steroids were beneficial in managing posterior uveitis, but had a high rate of relapse.5 In a prospective study following 50 patients with BD and posterior uveitis, 8/20 (40%) and 12/20 (60%) patients achieved complete and partial remission, respectively after an 8-week infusion of infliximab. 14/20 (70%) patients achieved complete remission after 32 weeks. 6/20 (30%) of these patients relapsed between weeks 8 and 21.6
Supplementary information

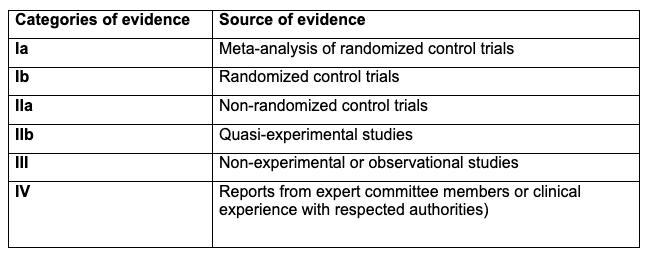
Table 1. Categories of evidence based on ‘Oxford System’ classification of levels of evidence.1

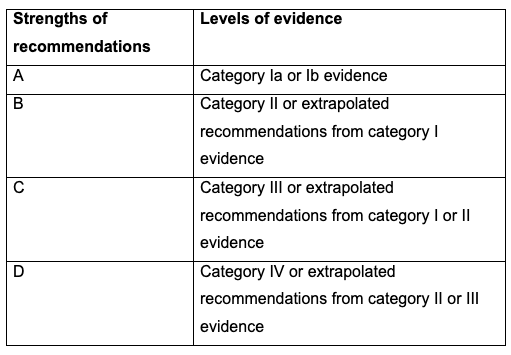
Table 2. Strengths of recommendations based on respective levels of evidence according to the ‘Oxford System’ classification.1

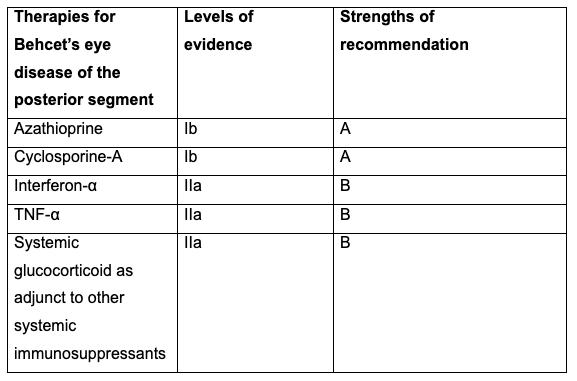
Table 3. Levels of evidence and strengths of recommendations for management of posterior segment Behcet’s eye disease.1
References
- Hatemi G, Christensen R, Bang D, et al. 2018 update of the EULAR recommendations for the management of Behçet’s syndrome. Ann Rheum Dis 2018; 77: 808-818.
- Tugal-Tutkun I, Onal S, Altan-Yaycioglu R, et al. Uveitis in Behçet’s disease: an analysis of 880 patients. Am J Ophthalmol 2004;138:373-80.
- Takeno M. Positioning of apremilast in treatment of Behçet's disease. Mod Rheumatol. 2020;30(2):219-224. doi:10.1080/14397595.2019.1696504.
- Hatemi G, Mahr A, Ishigatsubo Y, et al. Trial of Apremilast for Oral Ulcers in Behçet's Syndrome. N Engl J Med 2019;381:1918-1928.
- Khalil HE, El Gendy HA, Youssef HA, et al. The effectiveness of intraocular methotrexate in the treatment of posterior uveitis in Behçet’s disease patients compared to retrobulbar steroids injection. J Ophthalmol 2016; 2016:1678495. doi: 10.1155/2016/1678495.
- Garf AKE, Shahin AA, Shawky SA, et al. Efficacy of infliximab in refractory posterior uveitis in BD patients. Egypt Rheumatol 2018; 40: 93-97.
- H. Direskeneli, Autoimmunity vs autoinflammation in Behcet's disease: do we oversimplify a complex disorder? Rheumatology, Volume 45, Issue 12, December 2006, Pages 1461–1465.
- Davatchi F. Diagnosis/Classification Criteria for Behcet's Disease. Patholog Res Int. 2012;2012:607921. doi:10.1155/2012/607921


