


Amblyopia is a reduction in overall vision due to anisometropia, strabismus, high refractive error or cataracts in early childhood. In most cases, the patient has one eye with reduced vision, thus giving the colloquial “lazy” title. This term assumes a passive indifference on the poorer-seeing eye, and monocular treatment (patching, atropine or filters) have been the primary treatment for hundreds of years.1 Although many practitioners focus solely on the reduced acuity, amblyopia is a multifaceted condition presenting challenges in spatial awareness, oculomotor control, accommodation and visual information processing.
Underlying causes
Traditional treatment of amblyopia involves patching the better-seeing eye. The PEDIG study showed that for children with moderate amblyopia (20/40 to 20/80), two hours of patching a day (with near activities) was just as effective as six hours.2 This was a great relief to many patients! However, patients with very poor acuity in the amblyopic eye often find any amount of patching uncomfortable. In addition, acuity may worsen over time after discontinuation of therapy. Monocular treatment falls short in 15-50% of patients2 because it does not consider the underlying cause of the amblyopia.
- Anisometropia is a large difference in prescription between the two eyes. Optical correction is the first-line treatment for this condition, but that treatment alone may not fully correct it. A high prescription in one eye can cause that image to appear significantly larger, making it hard for the brain to fuse the images from both eyes. When that happens, the brain usually chooses to suppress the larger or blurred image.
- Strabismus is a misalignment of one or both eyes, horizontally or vertically. This results in double vision until the brain chooses to suppress the image from the turned eye.
- High refractive error is a large (usually far-sighted) prescription in both eyes. Without optical correction, the patient expends significant effort to focus, which often causes an eye to drift inward. This results in double vision until the brain chooses to suppress the image from the turned eye.
- Congenital cataract is a clouding of the infant’s lens inside the eye. This causes deprivation amblyopia, where the eye with the cataract does not receive the same stimuli for development as the fellow eye. Early surgical treatment is critical for visual development, but additional therapy may be indicated to improve the interaction between the two eyes.
In these cases, the amblyopia develops as a response to poor binocular function. Instead of being “lazy,” the poorer-seeing eye is being actively ignored. This creates a bully-like situation, where the better-seeing eye is causing the brain to suppress the poorer-seeing eye. Even if the acuity improves with patching therapy (for example), it does not necessarily solve the suppression problem. When the patch is removed, the patient reverts to the previous adaptation, primarily using only the non-amblyopic eye. Therefore, monocular treatment may fail, and visual acuity can regress after treatment ends.
Binocular treatment options: MFBF
Recent ophthalmological studies have shown that amblyopia is primarily a binocular problem.3,4 EE Birch’s 2013 paper states, “we have come to view binocular dysfunction as the primary deficit and the monocular visual acuity deficit as secondary. In this framework, patching, with or without perceptual learning treatment, treats the secondary monocular visual deficits but does not directly address the primary binocular deficit.”3 Interestingly, behavioral optometrists have taken a binocular approach to amblyopia therapy for over fifty years.5-8
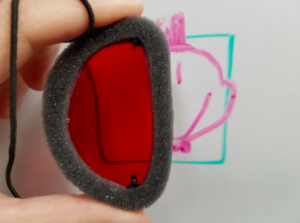
Binocular treatment involves engaging the poorer-seeing eye while the better-seeing eye is open. We call this treatment “monocular fixation in a binocular field (MFBF).”10 This is done by placing a colored filter over the better-seeing eye so that the visual target disappears. In most cases, a red lens is placed over the better-seeing eye, which causes red, pink and yellow colors to disappear. The amblyopic eye is therefore engaged in the activity while the non-amblyopic eye is still active. This can be utilized with pen-and-paper (dot to dots, coloring, word searches) and with electronic devices.4,9 With electronics, a red acetate sheet is placed over the screen, the the patient wears red-green glasses, with the red lens over the amblyopic eye. The non-amblyopic eye will see a black screen (red cancels green), and the amblyopic eye will see the details on the screen.

MFBF therapy is the treatment of choice for non-strabismic amblyopia. However, for patients with constant esotropia, practitioners should use extreme caution before initiating any anti-suppression therapy.
It is important to note that amblyopia is not solely a visual acuity problem. Studies show that these patients have deficiencies in stereoacuity (depth perception), gaze stability, oculomotor function (eye movement control) and fine motor skills.3 In fact, a study published last week indicated that amblyopes had a slower reading speed due to an increased number of forward saccades.11 Birch explains, “Amblyopia can reduce reading speed in natural, binocular reading by 20%-50% and negatively affect academic performance.”11
The right tools (and help) for the job
A behavioral approach to amblyopia works on acuity improvement through MFBF techniques, along with therapy for any co-existing deficiencies in visual function such as oculomotor control, accommodation (focusing), depth perception and fine visual-motor integration. To find a behavioral optometrist near you, visit the website for the College of Optometrists for Vision Development.
To bring your amblyopia therapy into the 21st century, you need the right tools. Red eye patches, as in the photograph above, can be purchased by vision care providers through the Bernell website. Red acetate may be purchased in craft stores, online or through Bernell. Bernell also offers many varieties of red-green glasses, including some with a strap for younger children.
Finally, consider joining VTODs on FB, a group for optometrists and vision therapists where we discuss all aspects of vision therapy and rehabilitation.
Resources
- Loudon SE, Simonsz HJ. The history of the treatment of amblyopia. Strabismus. 2005; 13:93–106.
- Repka, MX, et al. A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthamol. 2003 May; 121(5): 603-11.
- Birch EE. Amblyopia and binocular vision. Prog Ret Eye Res. 2013; 33:67–84.
- Birch EE. Binocular ipad treatment for amblyopia in preschool children. J AAPOS. 2015 Feb; 19(1): 6–11.
- Brock FW. Care of the amblyopic child. Am J Optom. 1967; 44: 44-55.
- Cook D. Optometric alternatives to amblyopia occlusion therapy. J Optom Vis Devel. 1995 Summer; 26: 71-75.
- Greenwald, I. Brock: A binocular approach to amblyopia therapy. J Optom Vis Devel. Summer; 26: 62-67.
- Sherman A. Treatment of amblyopia without full refractive correction or occlusion. J Behav Optom. 1995; 6:15-19.
- Hess RF, Thompson B, Black JM, et al. An iPod treatment of amblyopia: an updated binocular approach. Optometry. 2012; 83:87–94.
- Cohen AH. Monocular fixation in a binocular field. J Am Optom Assoc. 1981; 52:801-806.
- Birch EE. Amblyopia and slow reading. J AAPOS. 2017 Dec; 21(6): 442-444.


