


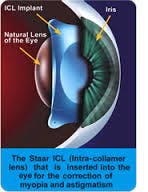
What is an implantable contact lens?
- A Visian Implantable Collamer Lens is planted behind the iris, but in front of the crystalline lens
- Made of Collamer that is naturally found within the body
- Corrects for the spherical component of the refraction
- In contrast to IOLs, Visian lenses can be folded and inserted through smaller incision sites without the need for sutures
- 95% of patients had vision of 20/40 or better
- Procedure is reversible and the lenses can be removed if patient is unsatisfied
- Has been approved in the states since 2005, with over 500,00 implants by surgeons completed
- Corrects myopia from -3.00 – -20.00 Diopters¹
Who is a good candidate?
- HIGH MYOPES!
- Patients between the ages of 21-45
- Patients with little or no astigmatism
- Patients with average or thin corneal thickness who may not be Lasik or PRK candidates
- Patients with sufficient large anterior chamber depth
- Patients with acceptable endothelial cell density
- Stable refractions with less then 0.50 diopters of change in two years
- Dry eye patients¹

Advantages of ICL vs Lasik
- Reversible
- No permanent changes made to the eye
- Less chance of regression for high myopes
- Correction for higher amounts of myopia
- No risk of corneal ectasia
- No risk of flap-related issues¹
Advantages of ICL vs PRK
- Quicker rate of recovery post surgery
- Correction for higher amounts of myopia¹
Patient Education
- Education on patient expectations for the iridotomy, possible headache, light sensitivity, and dull discomfort
- Risks are similar to cataract surgery: retinal detachments, macular edema, increased intraocular pressure, endophthalmitis
- Cataracts can be caused if surgeon touches the patient’s lens during surgery
- Halos my be increased due to iridotomy in low light conditions
Surgical Process
Several weeks prior to surgery, the patient must undergo a YAG laser iridotomy. The surgeon will use a laser to place two small openings at the edge of the iris to allow aqueous to flow from the back to the front of the eye.
The process of ICL implantation is similar to a cataract surgery except that the eye’s natural lens is not removed. The procedure is outpatient and the process for each eye is around 15 minutes.
O.D. Co-management Care
- Typically the ophthalmologist will follow-up 24 hours after the surgery to ensure intraocular pressure has not become elevated
- OD co-management may vary per surgeon, consult with your local surgeon for their preferred protocol
- ODs will be asked to document lens “vaulting” which is directly correlated to the size of ICL implanted²
Judging the “vault” of the lens is done by using a narrow slit lamp beam on the cornea and comparing the dark space between the ICL and the lens. Ideal vault is between 250-850 microns.
Vaulting
- Measurement is important for post-operative conditions like pupil block, IOP elevation, and iridotomy occlusion²
- Inadequate vault can lead to PSC cataracts and overvaulting can lead to increase in IOP²
- Picture C shows a vault of 50% while picture D has a vault of 200%²

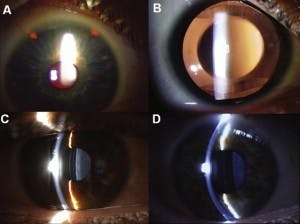
Picture C and D show vaulting of the lens using a narrow slit lamp beam 2
What’s new?
In March of 2014, the FDA endorsed the Visian Toric ICL for treatment. The FDA has not completed the approval process as of publishing; however, outside of the US, more then 100,000 toric ICLs have been implanted. The lens should correct up to -4.00D of astigmatism.
According to Starr Surgical’s website, U.S. clinical trials produced the following results:
“…210 eyes in 124 patients with a mean myopia of -9.37D and a mean astigmatism of +1.95D and an average age of 35. 12-month clinical outcomes show that 82% of the eyes were 20/20 or better uncorrected and 54% of the eyes were 20/16 or better.” ¹
Sources:
- ICL, Visian. “Visian ICL.” Visian ICL. Staar Surgical Company, 2006. Web. 11 Nov. 2015. <http://visianinfo.com>.
- Slade, Stephen, MD, and Richard Baker, MD. “LATEST ARTICLES.” A Surgeon’s Perspective on ICL: Implantable Collamer Lens. Slide & Baker Vision Center, 20 Aug. 2012. Web. 18 Nov. 2015. <https://www.visiontexas.com/houston/blog/detail/2012/08/20/a-surgeon-s-perspective-on-icl-implantable-collamer-lens.html>.


