


Femtosecond laser-assisted cataract surgery (FLACS) is a technologic advancement that has truly transformed how we approach cataract surgery, both with respect towards refractive cataract surgery, but also more complex cataract pathologies.
It specifically uses photodisruption laser technology to pre-treat the eye to make laser-created incisions as well as cleavage planes in the cataract, which allows for more consistent corneal incisions, astigmatism correction, capsulotomies, and also limits the overall amount of phacoemulsification energy needed. This technology can also be beneficial to select patients with corneal endothelial dystrophies, for which limiting the amount of energy used can sometimes mean the difference between one surgery or two.
PEARL #1: Optimize positioning to set yourself up for success
Patient selection is key. To optimize success, you’ll want to select patients that do not have conditions that may pose challenges for ideal positioning, cooperation, and docking for femtosecond laser assisted cataract surgery. Patients who have significant tremor, nystagmus, or have trouble laying flat are not ideal candidates.
Additionally, patients with anatomic challenges such as small palpebral fissures, deep-set eyes, or significant ocular surface irregularities (such as conjunctivochalasis, corneal/conjunctival scarring or pterygia) may prevent proper docking with the laser. I also do not consider any advanced glaucoma patients, patients with posterior polar cataracts or other known or suspected capsular compromise, patients with hypotony, or patients with significant blepharospasm or hemifacial spasm as appropriate candidates either.
Also, appropriate patients should all be able to dilate adequately preoperatively. I generally prefer a 5-mm capsulorhexis, so if they cannot dilate enough to allow for this, I prefer to make my rhexis manually. For patients who are borderline, I like to use pledgets soaked with phenylephrine/tropicamide/cyclopentolate and place this in the patient’s inferior fornix in the pre-operative area to get optimal dilation.
Some surgeons have also reported using FLACS for the capsulorhexis and phacofragmentation after the patient was already brought into the operating room with some sort of iris expander used prior to use of the femtosecond laser. Of course, these considerations are patient dependent, and using FLACS in poorly dilating patients may best be reserved for rare cases of trauma or subluxation where it allows for ideal rhexis formation in more challenging circumstances and is deemed the better option by the surgeon.
PEARL #2: Capsulotomy
When I was first learning how to do femtosecond laser assisted cataract surgery, I initially noted a higher relative incidence of tags despite having proper flat docking. I solved this by slightly extending the depth of penetration in my capsulotomy settings.
Additionally, any small persistent tags can be seen and gently broken when entering the eye with instilling initial lidocaine/Shugarcaine/phenylephrine or even viscoelastic instillation with intentionally targeting the influx of fluid towards the suspected/identified area of a persistent tag. I also use the cystotome to gently “check” that the rhexis is free by manually pulling the suspected “free” edges of the capsule centrally to ensure it is free 360 degrees.
If there are persistent attachments, it’s recommended to gently grasp the center of the freed capsule and with rotational forces, pull towards the apex of the cornea to avoid the creation of radializing capsular tears.
This video demonstrates one technique for checking to ensure the rhexis is complete and without tags with the cystotome.
Some surgeons, like myself, have had good success with using femtosecond laser for white cataracts, which can be very helpful in preventing the dreaded “Argentinian Flag sign” with anterior capsular rupture that may extend posteriorly.
However, with intumescent lenses, some surgeons are concerned about the liquified cortex extending into the aqueous with the free floating proteins limiting adequate transmission of the laser for complete capsulorhexis formation, which may result in persistent capsular attachments/tags that may extend into capsular tears. Personally, I find it easier to manage a tag in these cases, but this is surgeon dependent. Again, it’s important to use rotational forces in all of these cases to avoid radializing tears.
PEARL #3: Hydrodissection

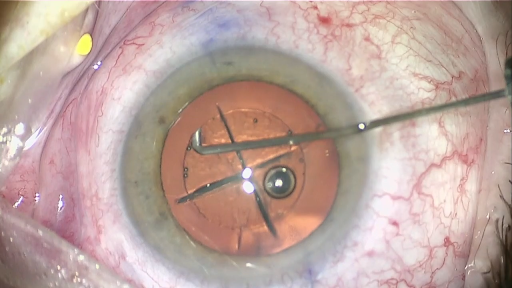
Figure 1: Hydrodissection
As phacofragmentation creates bubbles that can be more posterior in the lens, some advocate for grooving and cracking prior to hydrodissection, for surgeons who use the divide-and-conquer technique. This is meant to be done with a gentle rocking of the lens to gently move these bubbles anteriorly to prevent a posterior capsular blowout, which is thought to occur when additional retrolenticular pressure leads to a posterior capsular rupture.
For this reason, I consider posterior polar cataracts to be an absolute contraindication to FLACS. We know from Osher et al. that there is a 26% incidence of posterior capsular rupture with posterior polar cataracts (with some of these patients even having a partial absence of capsule as well). The posterior capsules in these patients are not normal, so you want to avoid any additional possible pressure or manipulation that may lead to a rupture. I would also exercise caution when a patient has a very dense posterior subcapsular cataract.
I have tried both hydrodissection prior to and after initial cracking, however I no longer routinely use the divide-and-conquer technique. Ultimately both methods can work well, as long as careful attention is made to coax posterior bubbles away from the posterior capsule during hydrodissection.
If you are concerned about creating significant retrolenticular pressure, it’s important to note that using the small-diced cubes as your phacofragmentation pattern (that may be recommended for those extremely dense cataracts typically found in our elderly population) increases the formation of these bubbles. Using the pie-cut fragmentation pattern and limiting or even foregoing the cylinders will limit the formation of these retrolenticular bubbles, although that will not soften the cataract as much as the former options.
Figure 2 demonstrates common phacofragmentation patterns, from right to left: quadrants with cylinders, sextants, and small diced cubes.

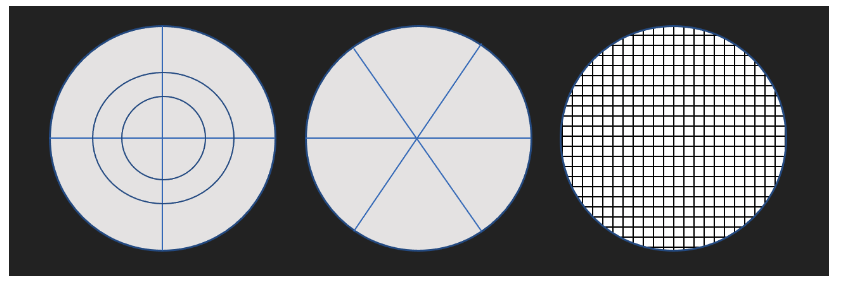
Figure 2
Ultimately, surgeons should use what is best in their hands and customize it for their patients’ needs.
I prefer to use a simple cleavage pattern that divides the cataract into four quadrants. I find this allows me to chop more “cleanly.”
In this video, I am using hydrodissection to prolapse and flip the lens up, which allows me to chop along the cleavage plane to minimize phacoemulsification energy. Most CDE is used while sculpting, so the more you can break up the cataract manually, the better.
📝
Watch the surgical video!
Sign up for our newsletter and get access to this and many other resources.
Pearl #4: Addressing astigmatism
For my patients who are not quite toric candidates, but still have a significant amount of astigmatism, I prefer to use limbal arcuate incisions to optimize refractive outcomes.
In my hands, I find greater success in minimizing residual astigmatism by way of limbal arcuate incisions after having adjusted my settings so the laser transmission begins at the anterior cornea, allowing me to open up my LRI’s with a Sinksey hook. Although LRI’s are typically programmed to be done intrastromally, they can be adjusted so your settings are brought more anteriorly. This allows the incisions to be opened up and potentially offer greater effect.
For larger amounts of astigmatism, I prefer using a toric lens implant. I typically like to mark my patients (while they are sitting up to account for cyclotorsion) in the preoperative area with a RoboMarker, which is a pre-inked, sterile self-leveling marking system. When using the femtosecond laser, I like to set this marker at 180 degrees, so I can use these markings to adjust where I want to place my LRI’s. I then will place a small and shallow 15 degree marking to serve as an indicator for where I want my toric lens to be positioned.
Pearl #5: Cortical clean up
Many surgeons note that the cortex feels “gummier” when removing it post-FLACS phacofragmentation. As with standard phacoemulsification, I opt for taking out subincisional cortex first. Subincisional cortex is generally thought to be the most challenging area, and removing it first is typically the safest time to do so, as the rest of the cortex is protecting the rest of the bag.
If some of the cortex is “too gummy” remove with ease, you can use your hydrodissection cannula to hydrate the cortex to make it easier to remove. Sometimes with very stubborn cortex, I will insert the lens first and rotate it a bit to encourage the last bit of cortex to be removed. This way, the lens is already safely in the bag as well.
Final thoughts on FLACS
In summary, femtosecond laser-assisted cataract surgery is a fantastic tool to have in your armamentarium, especially for unique and challenging cataract cases, such as traumatic, very dense, or white cataracts. It’s also an exceptional tool for treating patients with astigmatism. And although there have been some surgeons who argue that it doesn’t necessarily lead to faster recovery for patients, I do believe that by selecting the appropriate phacofragmentation patterns for the right types of various cataracts, it helps to reduce cumulative dissipated energy (CDE).
Higher CDE means more energy is dissipated in the eye, which generally leads to a longer surgical recovery time. Flip and chop is my preferred technique for cataract surgery, and while of course you can do this method manually, it is made even easier to do with cleavage lines already made with FLACS. Generally, the pieces come up quite easily and I find I can often finish with mostly manual chopping and aspiration. If FLACS has made the cataract gummier, I slide my chopper under the rhexis edge, go behind one of the quadrants, and gently lift it up towards my phaco tip.
However, there is a learning curve with FLACS and to optimize your success with it, I highly recommend learning and trying the various methods to find out what works best in your hands. Ultimately, this is a technology that patients are becoming more and more familiar with, and it’s helpful if you can feel comfortable in offering this to your patients as well.


