


Dry eye disease (DED) is a multifactorial disease of the tears and ocular surface that results in tear film instability, symptoms of discomfort, and visual disturbance accompanied by potential damage to the ocular surface.1 Despite the multifactorial nature of DED, the current body of evidence has clearly elucidated excessive tear evaporation as a key driver,2 with up to 90% of cases having an evaporative etiology (Figure 1).3-5 Presently, there are no prescription drops available that target excessive tear evaporation,6-9 constituting a considerable shortfall in the current DED treatment armamentarium.

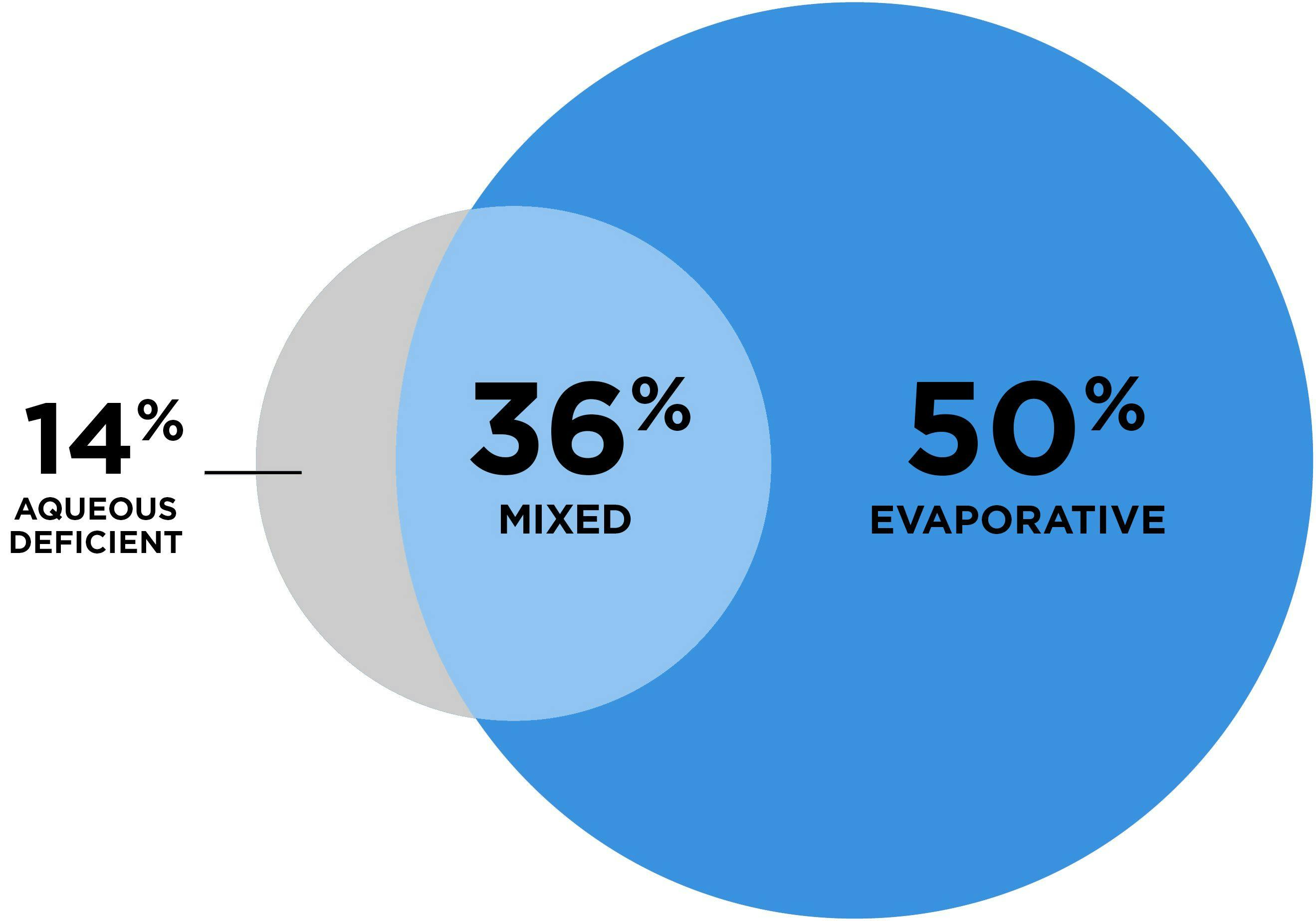
Figure 1. Classification of DED according to underlying cause(s)3
As one of the most prevalent medically treatable eye diseases seen by eye care professionals,2,10 DED has emerged as a growing public health concern. DED conveys a socioeconomic burden that interferes with quality of life, including visual disturbance, ocular discomfort, reduced vitality, eye pain, and limitations in performing daily activities.2
The COVID-19 pandemic has further intensified the urgency to address the growing burden of DED. While the impact of the pandemic on DED is still an active area of research, it has been postulated that new onset or worsening of symptoms may be associated with such factors as rising screen time in an increasingly digital world,11 chronic sequelae associated with contraction of SARS-CoV2,12 and increased tear evaporation following prolonged mask use.13 To effectively combat the rising tide of DED, it is now more critical than ever to consider etiology and the mechanisms underlying a patient’s DED, emphasizing the need for development of prescription anti-evaporative drop therapies that address this root cause of the disease.
Pathophysiology of evaporative DED
Meibomian gland dysfunction (MGD) is widely recognized as the primary driver of evaporative DED.3-5 Together, a growing body of population-based studies strongly suggest that among patients with DED, a large majority—roughly 70%-90%—display evidence of MGD.3-5
Meibum is a complex lipid secretion of the meibomian glands that forms the tear film lipid layer, which protects the ocular surface as an essential part of a healthy tear film.14 MGD is characterized by changes in meibum composition and reduced meibum secretion with resultant breakdown of the tear film lipid layer.15,16 MGD is progressive, with increasing gland atrophy and dropout as well as reduction of meibum quality and quantity as patients age.16 MGD causes unchecked evaporation and tear film instability, triggering a self-perpetuating cycle of ocular surface damage, downstream inflammation, and worsening of DED symptoms, as shown in Figure 2.2,17

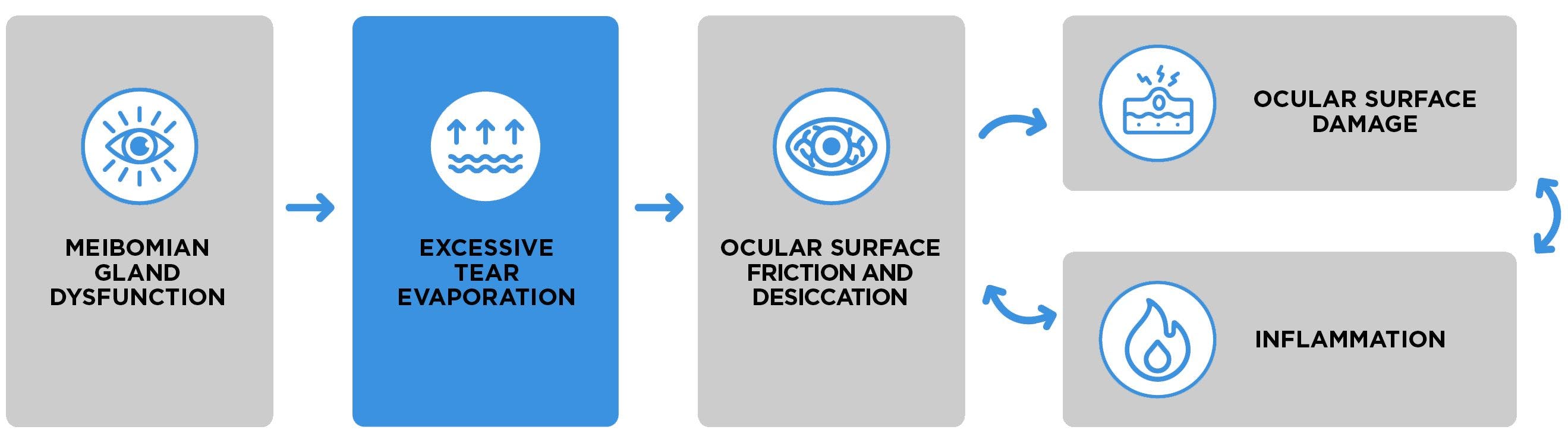
Figure 2. The vicious, self-perpetuating cycle of evaporative DED.
Desiccation stress and downstream inflammation
Following breakdown of the tear film lipid layer and accelerated rates of evaporation, desiccation stress further complicates the course of DED. Desiccation stress occurs when tear evaporation exceeds tear production, leading to drying and damage of the corneal epithelium; cell apoptosis; upregulation of innate and adaptive inflammatory pathways; and loss of goblet cells and tight junctions.17 These events ultimately contribute to a loss of ocular surface homeostasis, as supported by recent literature, including research utilizing a murine model of desiccation stress.18
Current treatments: Benefits and challenges
Directly managing excessive evaporation downstream of MGD could potentially help address the cycle of ocular surface damage and inflammation that chronically persists in patients with evaporative dry eye. Current devices and procedures—including intense pulsed light,19,20 thermal pulsation,21 and hot compresses—that help address a key upstream driver of evaporation, MGD, have shown evidence of providing at least short-term relief from DED signs and symptoms.
Current prescription treatment options are effective at targeting two of three potential contributing factors to DED: tear insufficiency and inflammation. However, anti-inflammatories and tear stimulators may be insufficient to resolve symptoms of DED,22 and the side-effect profile associated with topical steroids limits their potential use to a 2-week course.7 These limitations are further compounded by high discontinuation and low adherence rates to available therapies. Real-world analysis of cyclosporine and lifitegrast usage found that over 60% of patients with DED discontinued these treatments within 12 months of initiation.23 This demonstrates a significant unmet need for additional DED treatments that address the underlying etiology of the disease.
Conclusion
Excessive tear evaporation continues to hinder DED treatment efforts. No prescription drops targeting evaporation are currently available.6-9 As long as excessive evaporation continues to occur, signs and symptoms of DED may chronically persist.
Dr. White is a paid consultant of Bausch & Lomb Incorporated or its affiliates.
BLNP.0005.USA.23
BLNP.0005.USA.23
