



Optometrists and ophthalmologists today practice on the front lines of the chronic disease epidemic. Regardless of practice modality, most eye care practitioners are likely to encounter the ocular manifestations of chronic systemic disease on a daily basis—including cardiovascular disease (CVD). Whether it’s sight-threatening retinopathy, anterior segment disease, or a secondary glaucoma, eyecare providers must be knowledgeable and confident in managing the ocular sequelae these patients often present with.
In addition to retinopathy, ocular emergencies like neovascular glaucoma (a secondary glaucoma) can also present to your office, and occur more frequently in patients with uncontrolled chronic disease—including CVD. Atherosclerosis, congestive heart failure, heart attacks, and strokes can also significantly alter a patient’s quality of life and occur more frequently among CVD patients.
In this article we’ll explore the ocular manifestations of chronic uncontrolled CVD and discuss specific management strategies for patients presenting with secondary neovascular glaucoma.
Understanding how your front-line colleagues approach glaucoma is more important than ever. Download Eyes On Eyecare's free 2023 Glaucoma Report to see how your peers diagnose, treat, and manage this condition!
The prevalence of cardiovascular disease (CVD)
Since the turn of the century, the prevalence of cardiovascular disease (CVD) has significantly increased worldwide. Nearly half of all American adults have some form of cardiovascular disease. CVD commonly manifests in conjunction with hypertension (HTN), metabolic syndrome, and/or diabetes mellitus (DM). These conditions are all known to compromise systemic circulation—eventually causing end-organ damage (including the eye and visual system). One out of every four deaths in the U.S. is linked to CVD. It is also the leading cause of mortality in the U.S.
According to the American Heart Association, almost half of all U.S. adults (over 116 million) are affected by hypertension. The CDC reports that over 30 million Americans today (~one in 10) are affected by diabetes, with ~95% being type 2 (T2DM). There are also over 84 million Americans currently with pre-diabetes.
In other words, one out of every three adult patients you see in clinic will likely have either prediabetes or overt T2DM. While the pathophysiology of diabetes mellitus begins as a disease of metabolic dysfunction, the microvascular/cardiovascular system becomes compromised in the later stages of the disease process (e.g., diabetic retinopathy). The prevalence of T2DM is expected to nearly double by the year 2030.
The potential for adverse ocular sequelae is significantly higher among patients with CVD. Ophthalmologically, we are mostly concerned with sight-threatening retinopathy and the further downstream sequelae of these conditions—including neovascular glaucoma. Patients presenting with retinopathy have a significantly greater risk of CVD-related mortality (up to six times higher).
The pathophysiology of neovascular glaucoma
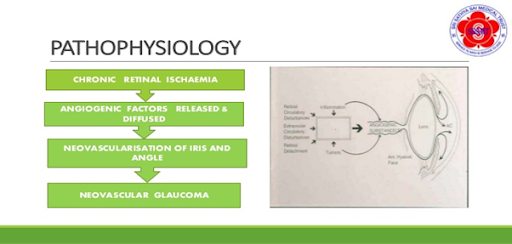
When CVD/HTN/DM is initially diagnosed, patients are typically asymptomatic for any systemic or ocular symptoms, sometimes for years or even decades. As systemic circulation is insidiously restricted, the eye is slowly “choked off” from an adequate supply of oxygen and other key nutrients. Over prolonged periods of hypoxia and compromised circulation, the body starts to produce a molecule called vascular endothelial growth factor (VEGF) in excess, including within the eye. It’s basically the retina’s way of saying “hey, we still need to breathe up here!” despite insufficient circulation from restricted blood vessels (CVD/HTN) or excess blood glucose (DM).
When excess VEGF is produced within the eye, the existing blood vessels become hyperpermeable or “leaky” in an attempt to deliver more oxygen to the ocular structures. This scenario is considered a “pro angiogenic/pro growth” state. While this may sound like a good idea initially, serious sight-threatening ocular complications can occur—primarily proliferative retinopathy and neovascular glaucoma (NVG).
NVG is considered a secondary glaucoma and results from the neovascularization of the iris (NVI) with subsequent neovascular occlusion of the anterior chamber angle (NVA). This scenario results in the rapid elevation of intraocular pressure (IOP), sometimes greater than 60mmHg.
NVG occurs when the trabecular meshwork is partially or completely blocked off from the abnormal growth of new blood vessels within the anterior chamber angle. This condition leads to angle closure and is considered an ocular emergency requiring immediate treatment on behalf of the astute clinician.

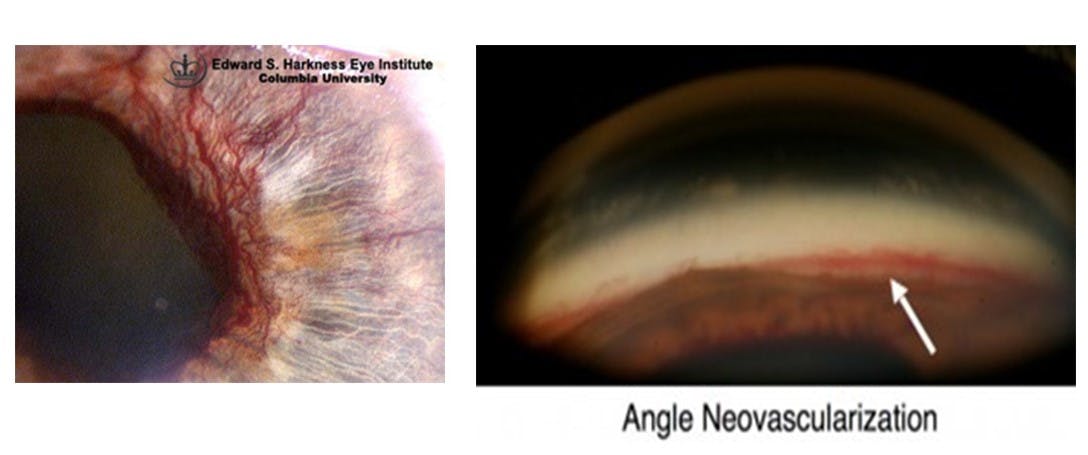
Fig. 1 NVI First defined by Dr. George Coats3 in relation to CRVO as thrombotic or congestive iris rubeosis and later termed NVG by Dr. Daniel Weiss.6 Classic depiction of iris neovascularization (left). Retinal ischemia creates a stimulus for pro-angiogenic growth factors, which result in NVI at the pupillary border further invading the anterior chamber angle, disrupting aqueous outflow and elevating IOP.3-7 NVA noted on gonioscopy (right).
Typically, primary open-angle glaucoma (POAG) and normal tension glaucoma (NTG) are often slow, painless, progressive diseases that takes place over years to decades. POAG pathogenesis is primarily thought to be caused from elevated eye pressure or ocular ischemia, while NTG pathogenesis is more likely attributed to ocular ischemia.
Patients who experience acute angle closure from NVG, however, will often complain of severe ocular pain, photophobia, and hazy/cloudy vision. These patients can be at risk of going completely blind in a matter of hours to days, and require immediate treatment. NVG can cause irreversible, rapid vision loss and will typically result in patients being left with light-perception vision. This devastating aftermath can occur within hours to days.

Top three causes of neovascular glaucoma
Most (~95%) of all NVG cases are caused by conditions that cause retinal ischemia.5 (eg. T2DM). The most common causes of NVG are proliferative diabetic retinopathy (PDR) and central retinal vein occlusion (CRVO).3 PDR is the primary cause of NVG—if abnormal angiogenesis is occurring in the back of the eye (retina), it can also occur up front (iris). Both PDR and CRVO are devastating consequences of poorly controlled chronic disease, and significantly contribute to the burden of blindness in the world.3-6

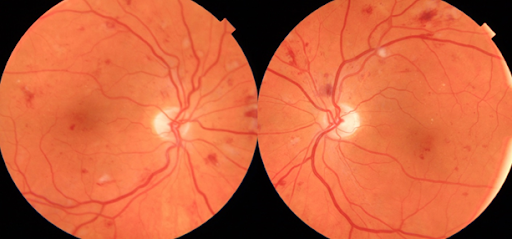
Fig. 2 Severe non-proliferative diabetic retinopathy in both eyes in a 65 y/o female with uncontrolled T2DM and HTN. Photos courtesy of Kevin Cornwell, OD.
Central retinal vein occlusion (CRVO)
The central retinal artery and vein bring blood to and from the eye, respectively. Patients who suffer from CVD/HTN/DM tend to have “thicker,” more viscous blood that is prone to clotting. When blood clots form within the central retinal vein, the outflow of blood is impeded from the eye and a state of hypoxia/ocular ischemia occurs (as new oxygen cannot be adequately delivered).
Patients with CVD/HTN/DM also tend to have stiffer-than-average arteries. In addition to a blood clot “stopping traffic” within the central retinal vein, CRVOs can also form by venous mechanical compression from the retinal arteries as they traverse adjacently to the retinal vein in the eye. CRVO is the second most common cause of NVG and carries the reputation of causing a “90-day glaucoma.” CRVO causes a significant level of ocular/retinal ischemia and contributes to the formation of NVI/NVA and subsequent NVG within three months of onset. It is therefore prudent to maintain close observation of these patients via gonioscopy and IOP checks to rule out NVI/NVA.

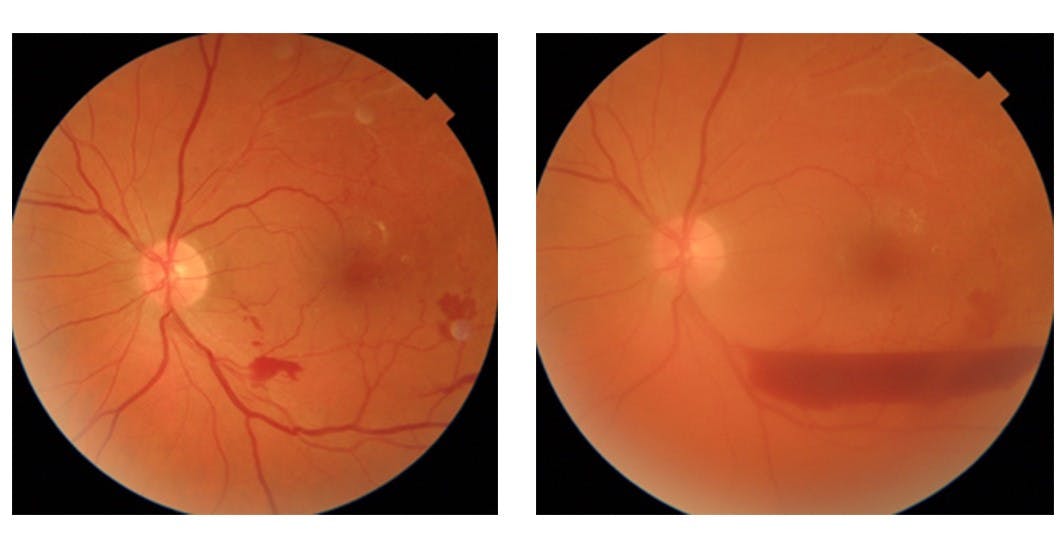
Fig. 3 Central Retinal Vein Occlusion of the left eye in a 52 y/o female with uncontrolled HTN and longstanding history of smoking (left). This patient was lost to follow up, then later presented with secondary vitreous hemorrhage in the same eye three months later (right). Photos courtesy of Kevin Cornwell, OD.
Ocular ischemic syndrome (OIS) and proliferative diabetic retinopathy (PDR)
Ocular ischemic syndrome (OIS) has also been shown to cause NVG and typically presents similar to PDR. This condition is also referred to as carotid artery occlusive disease (COAD). One key difference between OIS and PDR is that OIS will have a clinical presentation that is significantly asymmetric (worse on the side with the greatest carotid occlusion/ischemia) whereas PDR is almost always more symmetric/bilateral.
Patients with OIS can present with mid peripheral retinal hemorrhages, cotton wool spots, and a paradoxically low IOP (decreased aqueous production from hypoperfusion of ciliary body). Patients will also present with symptoms of moderate ocular pain and photophobia, with an accompanying iritis. These symptoms may improve slightly upon lying down (increased ocular perfusion). Patients with PDR are also more likely to be completely asymptomatic unless they have macular edema.
Enhancing care for patients with NVG
In order to ensure that patients presenting with NVG receive the best possible care, it is important for eye care practitioners to have a strong clinical skill set. Having a thorough understanding of the disease process along with the vast array of treatment modalities can help the patient avoid significant, irreversible vision loss.
These five points outline a systematic approach to the diagnosis, treatment, and management of NVG.
- High clinical suspicion
- Patient education
- Communication between providers and quick referral
- Prompt treatment
- Appropriate follow-up
1) High clinical suspicion
It is crucial to be on high alert for NVG anytime a patient with uncontrolled CVD presents to you.3-5 It is good practice to assume that every one of these patients has some form of NVI, NVA or retinopathy—until proven otherwise by the clinician. Always check both eyes for asymmetry and comparison. NVI typically presents with tiny red “buds” around the pupillary ruff and commonly precedes overt NVG. Always assess this area before dilating the patient as early detection is key. If you suspect you see NVI (and not normal physiological pigment which is browner in color), you must immediately perform gonioscopy to rule out NVA. Patients with NVI/NVA will not necessarily have an elevated IOP reading on initial presentation.
Taking a thorough case history can also help with your NVG detection and diagnosis. Is the patient asymptomatic? Are they experiencing blurry vision, acute ocular pain and/or photophobia? Are both eyes affected or just one eye? Patients are typically asymptomatic in the initial stages of NVG while late-stage NVG will typically present with pain and photophobia.
Patients with uncontrolled NVG may also present with blurred vision and pain due to microcystic corneal edema, severe iritis, and/or hyphema. In these patients where a view into the eye may be difficult, the use of a B-scan for posterior exam may be necessary (e.g., to rule out tractional retinal detachment)
2) Patient Education
It is important to explain the clinical findings to patients using basic layman’s terms. Words like “excess vascular endothelial growth factor” are likely to fly right over their heads and further frustrate/confuse them. The better they understand their condition and risks of irreversible vision loss, the more cooperative they’ll be with the management, treatment, and follow up protocol.
When the patient is on the same page, it helps them take ownership of their condition, while improving compliance with appropriate medical care.
3) Communication between providers and quick referral
It is vital to refer these patients immediately (same day STAT!) to a provider that is familiar and comfortable with treating NVG. This is a condition requiring multi-sub-specialty care. It is important for the success of the patient’s care to ensure access to both a retina specialist as well as a glaucoma specialist.
In some rural settings where ophthalmology may be farther away, optometrists will initially treat NVG with oral/topical IOP lowering agents while the patient waits to be seen by ophthalmology. Confirming insurance acceptance and patient transportation/location feasibility is also crucial to successfully referring NVG patients.
Ensuring the patient is evaluated in a timely manner will improve the odds of preserving their vision and avoiding the rapid glaucomatous optic neuropathy than can ensue over hours to days if their elevated IOP is left untreated.
4) Prompt treatment
Regardless of practice setting, patients presenting with NVG and elevated IOP need immediate in-office IOP reduction to protect and preserve their vision. Topical beta blockers (e.g., timolol), alpha 2 agonists (e.g., alphagan) and topical/oral carbonic anhydrase inhibitors (e.g., dorzolamide or acetazolamide/diamox) are all viable options to use in-office to immediately reduce the patient’s eye pressure.
Prostaglandins have a more delayed onset of action and are typically avoided with NVG. Prostaglandins can also further break down the blood-aqueous barrier and increase ocular inflammation—which is already present in NVG cases.
It is not uncommon for NVG patients to present with posterior synechiae to some extent. This occurs when adhesions between the posterior iris and anterior lens surface are formed secondary to the pro-inflammatory state of eyes with NVG. A complete iris bombe can even be seen during the advanced stages of posterior synechiae from NVG. In these cases, topical atropine or cycloplegia can be used in an attempt to break the synechiae and increase uveoscleral aqueous outflow.
Anterior chamber paracentesis is another effective technique to use to rapidly lower the patient’s IOP.
Patients with NVG have abnormally high levels of circulating VEGF within the eye and will likely also need treatment with anti-VEGF agents like Eylea, Lucentis or Avastin. Anti-VEGF agents are especially useful in the initial treatment of NVG patients where a clear view of the retina is not present (e.g., cataract, poor dilation, or vitreous hemorrhage). Anti-VEGF injections may be used as monotherapy or in conjunction with pan-retinal photocoagulation.
Currently, the scientific literature remains inconclusive as to the efficacy of NVG monotherapy using anti-VEGF treatment. Anti-VEGF therapy also increases the risk of tractional retinal detachment in patients with NVG and PDR.
Depending on the patient and practice setting, NVG is typically treated with PRP9-10 laser to further decrease the demand for oxygen within the ocular structures by ablating ischemic areas of the retina, PRP reduces the angiogenic burden.9 (Caveat: a clear view of the retina is required to perform PRP.)
While less urgent but still emergent, ordering a carotid doppler ultrasound is also necessary for patients whom you suspect may have had OIS. Co-managing OIS with a cardiologist and/or vascular surgeon is important as the patient may need possible treatment with a carotid endarterectomy.
Additional long term NVG treatment options also include the use of surgical glaucoma drainage devices (e.g., Ahmed valve12) and cyclophotcoagulation (CPC). Trabeculectomy tends to be less effective for NVG and further promotes ocular inflammation.5-11 CPC is an excellent treatment option for NVG treatment for eyes with limited potential for vision13 (e.g., end-stage glaucomatous optic neuropathy with persistent high IOP and ocular pain).
5) Appropriate follow-up
NVG patients must be observed closely to ensure their IOP/inflammation remains under control. These patients tend to be followed on a weekly or even daily basis initially while treatment options are considered and implemented. Follow-up intervals can then be extended after definitive treatment occurs and IOP begins to stabilize. Frequent dilated fundus evaluations are necessary to ensure the absence of new/progressive areas of iris/retinal/disc neovascularization.
Remember, early recognition and diagnosis is key. Repeat assessment of the angle via gonioscopy is also crucial. Early in the NVG disease process, your patient’s IOP may remain “normal” despite subtle findings of NVA or NVI. When these patients are caught sooner, eye care professionals are better able to intervene and prevent irreversible vision loss.

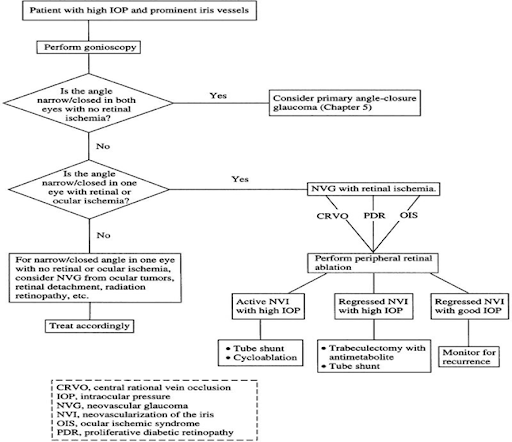
Fig. 4 Flowchart for NVG diagnosis and management 14
Final thoughts
Neovascular glaucoma is an ocular emergency with significant potential for rapid, irreversible visual loss. While this condition is caused by a myriad of ocular/systemic disease processes, proliferative diabetic retinopathy (primarily from T2DM) and central retinal vein occlusions are among the top causes.
Promoting routine eye care to at-risk patient populations can lead to earlier detection and treatment. Today’s chronic disease epidemic—including cardiovascular disease—continues to burden our patients and our health care system. It is vital for eye care professionals to understand the pathophysiology behind the myriad clinical manifestations of systemic disease.
It is also important to educate patients who are at risk for developing PDR, CRVO, and NVG before these unfortunate ocular complications occur. Smoking cessation counseling, as well as diet/lifestyle discussions for patients with CVD, HTN, diabetes, or pre-diabetes are crucial in preventing these conditions. Despite the practice setting, eye care practitioners today must maintain a keen eye in the detection of ocular sequelae from uncontrolled systemic disease. The best visual outcomes occur by preventing these ocular emergencies from occurring altogether; however, prompt recognition and appropriate treatment of the underlying etiology helps to preserve patients who are affected.
References
- Bullard KM, Cowie CC, Lessem SE, et al. Prevalence of diagnosed diabetes in adults by diabetes type – United States, 2016. MMWR Morb Mortal Wkly Rep. 2018 Mar 30;67(12):359-361.
- NCHS, National Health and Nutrition Examination Survey, 2015–2016.
- Rodrigues G, Abe R, Zangalli C, et al. Neovascular glaucoma: a review. International Journal of Retina and Vitreous.2016 ;2:26.
- Liao et al. Neovascular glaucoma: a retrospective review from a tertiary center in China. BMC Ophthalmology. 2016;16:14
- Sivak-Callcott JA et al. 00. Evidence-based recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmology.2001;39-41.
- Shazly TA, Latina MA, et al. Neovascular glaucoma: etiology, diagnosis and prognosis. Semin Ophthalmol.2009; 24(2):113-121.
- Havens SJ, Gulati V. Neovascular glaucoma. Dev Ophthalmol.2016; 55: 196-204.
- Saikumar SJ, Anup M, Nair A. Neovascular glaucoma. Kerala J of Ophthal.2018;30(3):172-77.
- Olmos LC, Lee RK, et al. Long-term outcomes of neovascular glaucoma treated with and without intravitreal bevacizumab. Int Ophthalmology Clin. 2011; 51(3): 27-36.
- Lüke J, Nassar K, Lüke M, Grisanti S. Ranibizumab as adjuvant in the treatment of rubeosis iridis and neovascular glaucoma-results from a prospective interventional case series. Graefes Arch Clin Exp Ophthalmol 2013;251(10):2403-2413.
- Takihara Y, Inatani M, Fukushima M, Iwao K, Iwao M, Tanihara H. Trabeculectomy with mitomycin C for neovascular glaucoma: prognostic factors for surgical failure. Am J Ophthalmol. 2009;147(5):912–8. 918 e911.
- Sun JT, Liang HJ, An M, Wang DB. Efficacy and Safety of Intraretinal Ranibizumab with Panretinal Photocoagulation followed by Trabeculectomy compared with Ahmed glaucoma valve implantation in neovascular glaucoma. International Journal of Ophthalmology 2017. 10(3) 400-405
- Zhou MW, Wang W, Huang WB, Chen SD, Li XY, Gao XB, Zhang XL. Adjunctive with versus without intravitreal bevacizumab injection before Ahmed glaucoma valve implantation in the treatment of neovascular glaucoma. Chin Med J (Engl) 2013;126(8):1412-1417.
- Vu CD, Alappatt JJ, et al. Neovascular Glaucoma. Ento Key. 2017. Research to Prevent Blindness, Inc.


