


These days, eyecare practitioners have a wide variety of ophthalmic imaging modalities at their disposal, often consolidated into multimodal imaging devices. These provide significant information regarding retinal anatomy and function, also assisting physicians in the diagnosis and management of ocular disease.
Knowing the appropriate clinical indication for each imaging modality is important to delivering quality patient care. In this article, we will take an in-depth look at one of the more recent and less mainstream of these modalities, fundus autofluorescence (FAF). After reviewing the basic principles of FAF, we will discuss its application in clinical practice.
Fundus Autofluorescence Imaging
While referenced in the medical literature since the 1980s, the use of FAF in routine eye care has increased significantly over the past 10 years. FAF is a noninvasive imaging method that highlights fluorophores in the retina, lipofuscin (LF) being the most dominant. As lipofuscin is a metabolic byproduct of RPE metabolism, FAF supplements anatomic imaging techniques by providing functional information about the retina and macula.
FAF uses a blue-light excitation beam that “excites” fluorophores, causing them to emit blue light. The resultant images are black and white, and findings are described as hyperautofluorescent (brighter signal) or hypoautofluorescent (darker signal). Normal tissue (figure 1) has a uniform hyperAF signal throughout the retina with the optic nerve and blood vessels appearing black as they do not contain fluorophores.

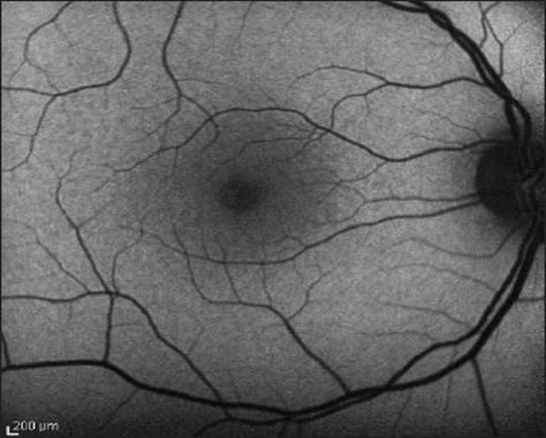
Figure 1: Fundus autofluorescence of a healthy eye. Note a dark optic nerve head and vessels.
Whereas lipofuscin gradually accumulates in the RPE due to photoreceptor metabolism as a part of natural aging, the metabolism of LF can be significantly altered in various ocular disease states (figure 2). FAF is commonly used to assess clinical changes with geographic atrophy in age-related macular degeneration (AMD), as well as characterize various retinal dystrophies. In general, hyperautofluorescence indicates “sick” RPE, where lipofuscin is poorly metabolized and begins to accumulate. Hypoautofluorescence can be considered “dead or dying” RPE, where the cells are unable to store adequate levels of lipofuscin.

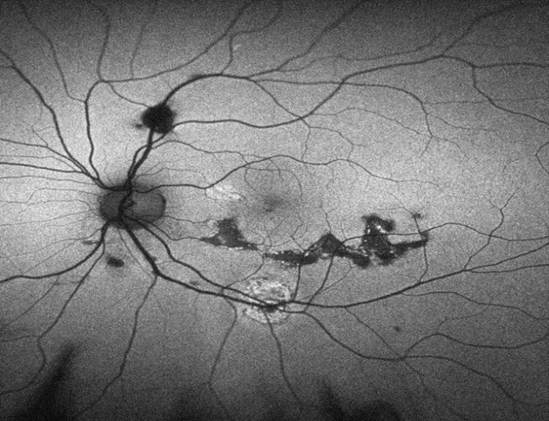
Figure 2: An abnormal fundus autofluorescence image showing areas of both hyper- and hypo- fundus autofluorescence. Note the area of pseudo-hypoFAF along the superior arcade that is due to pigment clumping blocking the signal, rather than representing a truly “sick” RPE.
These findings are fairly non-specific, and while they may assist in making a diagnosis, rarely do they do so alone. The monochromatic images produced via FAF lack the color information of a fundus photo or SD-OCT scan; however, they can still provide useful clinical information. Imaging via FAF is best used in conjunction with other modalities such as SD-OCT, fundus photography, or fluorescein angiography.
Table 1. Major causes for abnormal FAF
| Hypo Autofluorescence Absence or reduction of LF within RPE (black signal) | Hyper Autofluorescence Excessive LF accumulation within RPE (white/gray signal) |
|---|---|
| RPE loss or atrophy/geographic atrophy Hereditary retinal dystrophy Increased RPE melanin content Absorption from anterior structures Intraretinal fluid Migrated melanin-containing cells Intraretinal and subretinal fluid Fresh intraretinal and subretinal heme Fibrosis, scar, borders of laser scars Retinal vessels and ONH Luteal pigment Media opacities | Lipofuscinopathies (Stargardt, Best, AVMD) AMD (RPE at edge of geographic atrophy) Fluorophores outside RPE monolayer Intraretinal fluid Subretinal fluid (separation of PR from RPE) Subretinal macrophages containing LF (choroidal melanoma or high-risk choroidal nevi) Drusen in sub-RPE space Migrated RPE cells or macrophages with LF Older intraretinal or subretinal heme Choroidal vessel in presence of RPE loss Lack of absorbing material Depletion of luteal pigment (eg. mac tel) Displacement of luteal pigment (eg. CME) Optic nerve head drusen Artifacts |
Clinical Application of FAF
FAF can be useful in a handful of disease states. FAF is helpful to diagnose and monitor patients at risk for hydroxychloroquine maculopathy, and is part of the official screening guidelines (complementing SD OCT and/or multifocal ERG). Early findings may include mild perifoveal hyperFAF, which becomes hypoFAF in later stages. In diseases that are characterized by an abnormal accumulation of subretinal LF (e.g., Best’s disease, pattern dystrophy, Stargardt’s, or AMD), FAF can reveal striking hyperFAF, helping to confirm the diagnosis. In patients with geographic atrophy from macular degeneration, the FAF pattern can give important prognostic information providing a more detailed visualization than fundus photography alone.
Geographic atrophy that shows surrounding larger “banded” and “diffuse” hyperFAF patterns tend to have a higher rate of progression. In the Fundus Autofluorescence in AMD Study group, they showed that patients showing multiple large (>200 micron) areas of hyperFAF signal were at an increased risk of progressing to wet AMD. This study also confirmed the utility in FAF in identifying patients with higher risk for progressive geographic atrophy.
Fundus autofluorescence can also reveal RPE changes that other imaging modalities fail to highlight (e.g., chronic central serous retinopathy), as well as help differentiate retinal lesions (e.g., choroidal melanoma vs. benign choroidal nevus)
In summary, while not a game changer, fundus autofluorescence definitely enhances the quality of patient care, which is always the top priority. Viewing a FAF image provides a “metabolic map” of the retina and can help detect retinal pathology at earlier stages and enhance long-term visual outcomes. If you have access to FAF imaging technology, begin using it to monitor your patients with various retinal pathologies. You’ll soon find this imaging technique can help you better educate your patients on their ocular health while also assisting you in the clinical decision making process.


