


In this episode of Ready, Set, Retina, Roya Attar, OD, MBA, DHA, FAAO, joins Daniel Epshtein, OD, FAAO, to review a case report on a patient with proliferative diabetic retinopathy (PDR) that highlights how eyecare practitioners (ECPs) can utilize multimodal imaging to identify, diagnose, and grade DR.
Prevalence of diabetes and diabetic retinopathy
Dr. Epshtein noted that diabetes is a growing epidemic in the US, with around 11.6% of Americans (38.4 million) having diabetes and 38% of US adults (97.6 million) being pre-diabetic—making an overall total of 136 million people impacted by the disease.1
Diabetic retinopathy is an ocular complication of diabetes secondary to damaged retinal blood vessels and ischemia that can potentially progress to vision-threatening severity.2 It is currently the leading cause of blindness in adults, and approximately one in three diabetics develop some degree of DR during their lifetime.
A recent study found that in 2021, across all ages, an estimated 9.6 million people in the US live with DR; of these, 1.84 million live with vision-threatening DR.3 As this represents a significant portion of not only diabetics, but more generally the American population, it is crucial that ECPs can adeptly identify DR and recommend appropriate treatments to slow progression and potentially preserve patients’ vision.
Case report on diabetic retinopathy
A 70-year-old Black female patient presented to the clinic with a chief complaint of a floater in her left eye for around 1 week. Her history was positive for type 2 diabetes for about 26 years, with a current hemoglobin A1C (HbA1c) level of 7% and a blood sugar (fasting BS) level of 105mg/dL.
Other notable features in her medical history were heart disease and hyperlipidemia, and she had undergone amputation of both legs above the knee. Her best-corrected visual acuity (BCVA) in both eyes (OU) was 20/30. Dr. Attar mentioned that at a glance, on funduscopic examination, the patient’s right eye (OD) did not look severely impacted by the disease; however, upon closer inspection, it became clear that there were signs of advanced DR.
The image carousel (Figures 1 and 2) shows fundus photography of the patient’s right eye (and the quadrants highlighted by Dr. Attar as areas of concern).


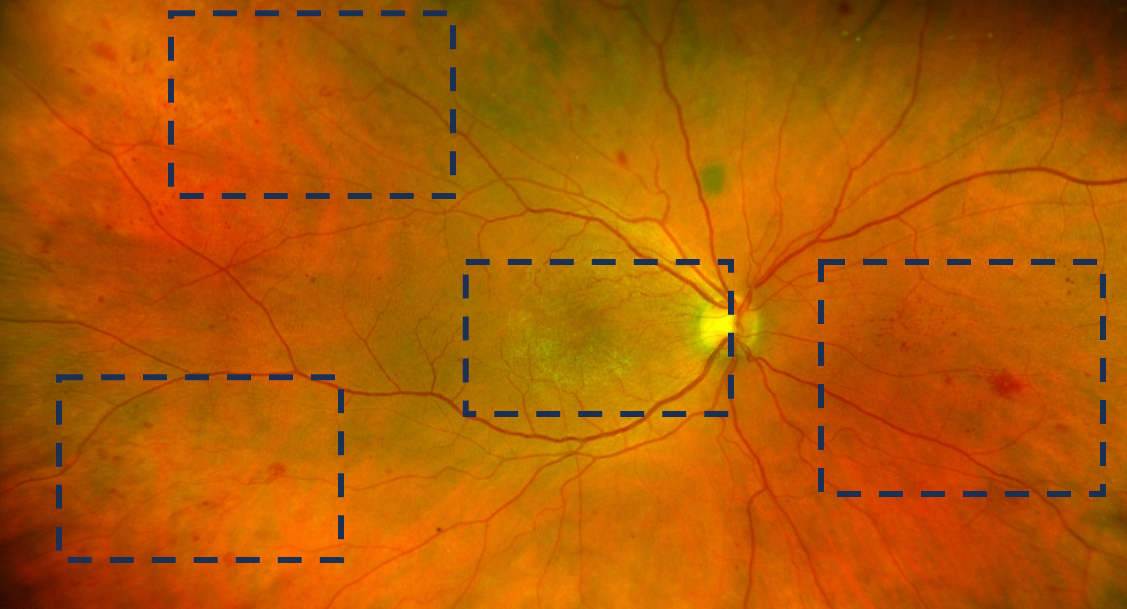
Images courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Evaluating DR patients with multimodal imaging
Dr. Attar explained that while the optic nerve looked relatively healthy, a closer look at the macular area showed rippling on fundus photography. While edema couldn’t be visualized via funduscopy, optical coherence tomography (OCT) revealed center-involving edema and an epiretinal membrane (ERM). Additionally, there were changes to the retinal pigment epithelium (RPE) consistent with age-related macular degeneration (AMD).
Figure 3 shows the prior fundus photograph of the optic nerve and macula OD with greater magnification, and Figure 4 is the corresponding OCT image, demonstrating center-involving edema, ERM, and RPE loss indicative of AMD.

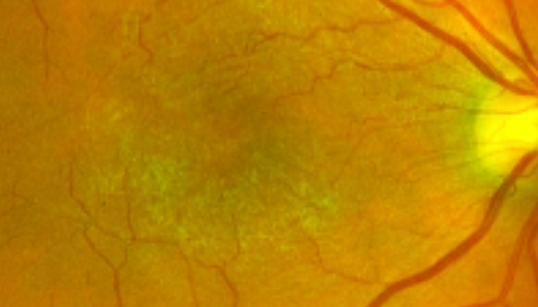
Figure 3: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.

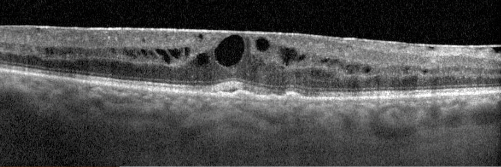
Figure 4: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Next, Dr. Attar focused on the three other quadrants from the funduscopic examination. In the periphery of the retina, there were intraretinal dot-blot hemorrhages—indicative of vascular disease, and possibly even neovascularization.
Then, further in the retinal periphery, there were additional intraretinal hemorrhages. This is notable, said Dr. Attar, because retinopathy from classic diabetes usually has its greatest impact within the posterior pole. Consequently, seeing signs of DR in the periphery suggests that the patient has progressive advancing disease, she added. The last quadrant showed a multitude of hemes and a white-centered heme (Figure 7).
Figure 5 demonstrates evidence of advanced DR OD with possible intraretinal microvascular abnormality (IRMA) and scattered retinal hemes in the periphery.

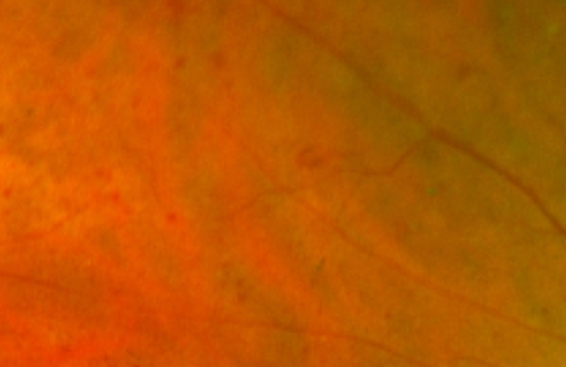
Figure 5: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 6 shows further signs of progressing diabetic retinopathy OD, with areas of IRMA as well as numerous dot and blot hemorrhages in the retinal periphery.

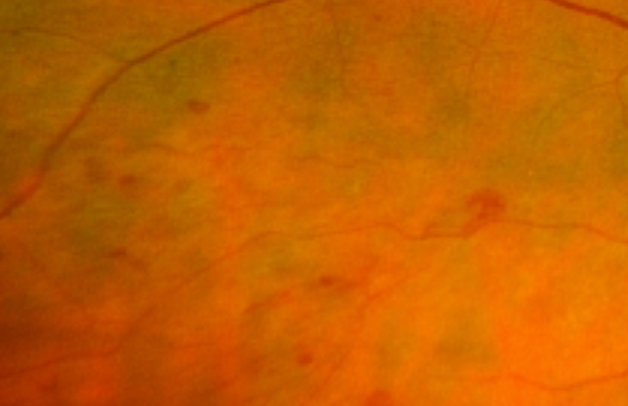
Figure 6: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 7 shows the final quadrant OD with multiple hemes, including a white-centered heme.

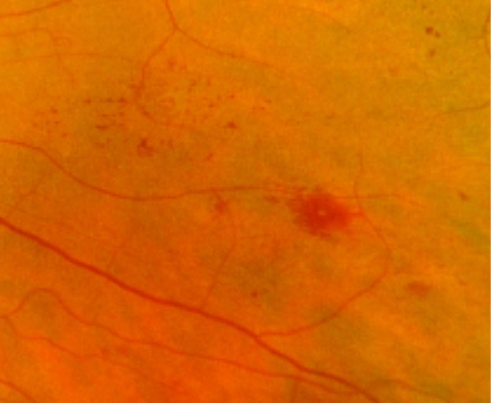
Figure 7: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Making the DR diagnosis with clues from multimodal imaging
Dr. Attar mentioned the “4-2-1” rule for diabetic retinopathy, in which severe non-proliferative DR (NPDR) can be identified if:3
- Hemorrhages or microaneurysms (or both) are in all four retinal quadrants
- Venous beading appears in two or more retinal quadrants
- Prominent IRMAs are present in at least one retinal quadrant
In this case, in the patient’s right eye, three of the four quadrants showed hemorrhages, venous beading couldn’t be appreciated from the fundus photograph, and the vascular anatomy had clearly changed in addition to the intraretinal hemes in her right eye.
Then, Dr. Attar showed a fundus photograph of the patient’s left eye (OS), which showed vitreous hemorrhage, a preretinal heme temporally, intraretinal hemorrhages, and blot hemes. Further, a closer inspection showed an area of neovascularization that confirmed the diagnosis of proliferative diabetic retinopathy.
The image carousel (Figures 8 and 9) shows the funduscopic examination in the patient’s left eye (OS) with vitreous hemorrhage, a temporal preretinal heme, intraretinal hemorrhages, and blot hemes.

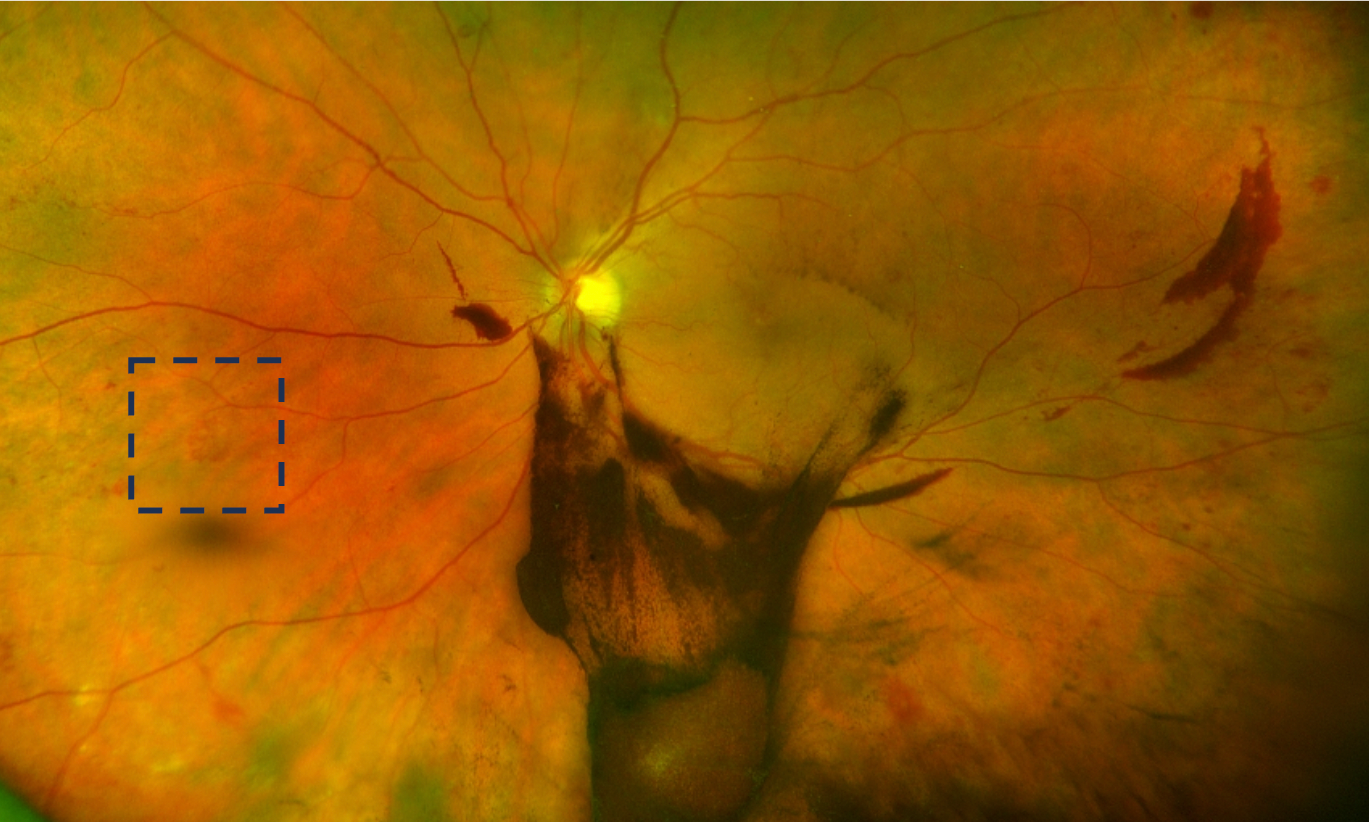
Images courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 10 is a close-up of the previous fundus photograph that highlights neovascularization OS.

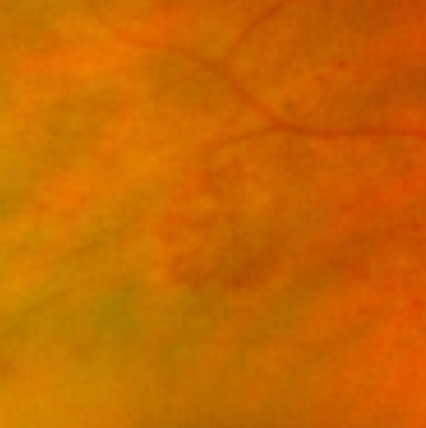
Figure 10: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 11 features OCT imaging of the left eye, showing no edema and RPE changes associated with AMD.

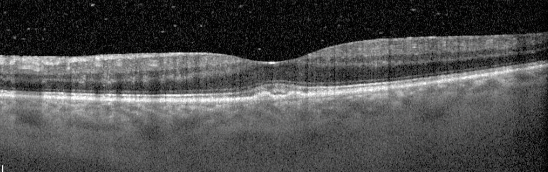
Figure 11: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
DR case report treatment and follow-up
After Dr. Attar confirmed the diagnosis of PDR for this patient, she was referred to a retinal specialist and scheduled for a 2-month follow-up appointment. During this time, the patient began undergoing anti-vascular endothelial growth factor (VEGF) injections and extensive panretinal photocoagulation (PRP).
At the 2-month follow-up appointment, the patient’s BCVA was 20/25 OU, but she still had significant retinal disease that could be visualized via ophthalmic imaging, noted Dr. Attar.
Figures 12 and 13 show fundus photographs from the 2-month follow-up appointment OD (top) and OS (bottom). Residual vitreous opacification from the resolving heme can be visualized in the left eye.


Figure 12: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.

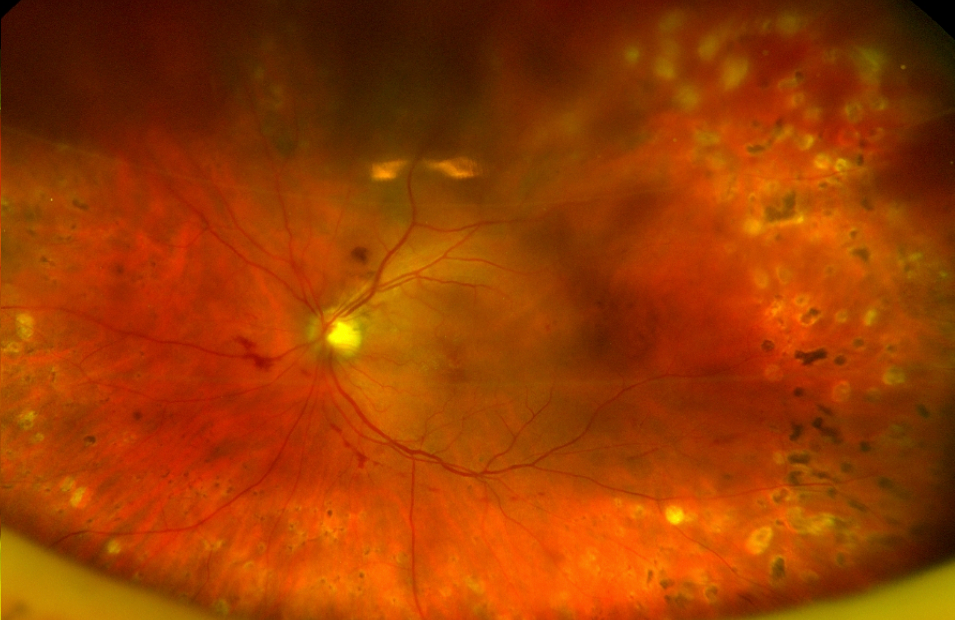
Figure 13: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 14 depicts OCT imaging of the right eye from the 2-month follow-up visit, demonstrating significant resolution of the edema, though there is still the presence of an ERM, RPE changes, and the beginnings of a macular pseudohole.

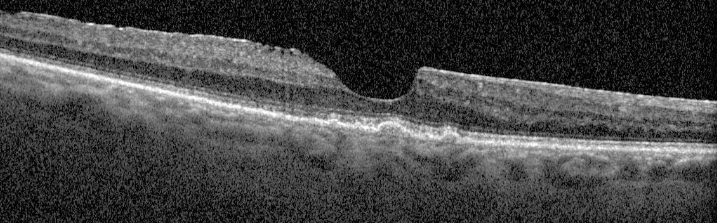
Figure 14: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Figure 15 represents OCT imaging from the 2-month follow-up visit from the left eye.

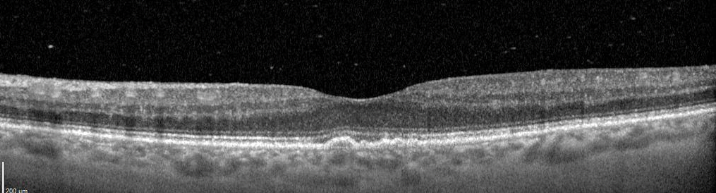
Figure 15: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Grading diabetic retinopathy
Next, Drs. Attar and Epshtein reviewed how to grade DR and the recommended follow-up intervals for varying levels of DR severity. Dr. Epshtein noted that there is a broad variety of presentations in DR, and while Dr. Attar’s patient had more severe DR in the form of PDR, more often, patients will present to clinics with mild to moderate DR.
Dr. Attar added that the International Clinical DR Severity Scale (seen below) is simply a guide, and that ECPs must consider each patient’s unique traits to make their decisions based on a comprehensive understanding of the patient’s ocular and systemic health to determine appropriate follow up.
For example, if a patient has no retinopathy but their diabetes is poorly controlled, if they have other poorly controlled vascular conditions, or if they are a high-risk patient, Dr. Attar stated that she would follow up with them sooner than the recommended 12 months.
Table 1 compares the International DR Scale (as opposed to the ETDRS scale used previously) to the recommended follow-up schedule for patients with DR.4
| Diabetic Retinopathy Grade | International Scale | Follow-Up Schedule |
|---|---|---|
| No apparent DR | No abnormalities | 12 months |
| Mild NPDR | Microaneurysm only | 6 to 12 months |
| Moderate NPDR | More than just microaneurysms but less than severe NPDR | 4 to 6 months |
| Severe NPDR | Any of the following (4-2-1 rule) and no PDR: severe hemorrhage in each quadrant, venous beading in two or more quadrants, IRMA in one or more quadrants | Refer in 2 to 4 weeks |
| PDR | One or more of the following: neovascularization, vitreous heme, or preretinal heme | Refer in 24 hours to 4 weeks |
Table 1: Courtesy of Wilkinson et al.
Considerations for following up with DR patients
Early detection and management of retinopathy is key, and being proactive communicates to patients the importance and severity of the condition, potentially motivating them to continue seeking treatment.
Dr. Attar emphasized that it is crucial to keep in mind that diabetic macular edema (DME) can be seen at any stage of DR—even in patients with mild NPDR. Additionally, center-involving DME should be referred for treatment within 2 to 4 weeks. Patients with non-center-involving DME can be considered for referral or close surveillance, depending on the specific case.
Dr. Epshtein noted that he tries to get OCT imaging in all patients with moderate NPDR and more advanced disease. Reiterating Dr. Attar’s point of looking at patients on a case-by-case basis, he explained that for diabetic patients, he looks not only at the absolute value of the HbA1c, but also at the trend in those values. If the patient’s HbA1c levels are trending upward, he is more likely to reduce the follow-up interval to monitor their symptoms more closely.
Putting the 4-2-1 rule into clinical practice
Dr. Attar mentioned that she has often discussed with colleagues how to best use the 4-2-1 rule when grading DR patients. In the case of this patient, there were clear indications that she had advanced DR because the retinopathy was not restricted to the posterior pole—it actually extended into the periphery.
Dr. Attar prefers to err on the side of caution, so she sets a tentative benchmark of 5 to 10 hemes in each quadrant before she considers the condition severe. Dr. Epshtein noted that he grades patients as having severe NPDR when there are 15 to 20 hemes per quadrant, though he also considers the non-ophthalmic risk factors as well.
Final thoughts
As diabetes continues to afflict a larger portion of the American population, ECPs will likely encounter more patients with DR, and will need to skillfully and promptly detect, grade, treat, and co-manage patients with diabetic retinopathy.
While some retinal specialists are electing to initiate treatments for patients with severe NPDR earlier in the disease course to prevent vision-threatening sequelae, Dr. Attar explained that many of her patients receive prophylactic PRP due to issues with insurance coverage and transportation. These restrictions make it difficult to maintain a consistent schedule of monthly or bi-monthly injections.
She added that many diabetic patients can get lost in the treatment process as they have to maintain appointments with a multitude of healthcare professionals. In the not-so-distant future, tele-ophthalmic diabetic screenings and artificial intelligence (AI)-based screening models may become everyday tools ECPs can utilize to improve eyecare accessibility for DR patients.2


