




Some of the most urgent and challenging clinical conditions that eyecare providers (ECPs) are apt to encounter involve acute inflammation of the anterior segment.
Why are these entities particularly challenging, you may ask? It’s because inflammation—particularly inflammation of an acute nature—carries a great deal of symptomatic “baggage.”
Most notably, these can include complaints such as swelling, hyperemia (of the conjunctiva and/or eyelids), possible photophobia, and, most of all, discomfort.
Dealing with unhappy and uncomfortable patients who may also have acute visual and/or cosmetic issues brings a greater sense of urgency than managing chronic conditions, where the impact felt by the patient is typically more gradual.
In this feature report, we’ll discuss some of these challenging clinical entities with greater specificity, including their therapeutic requirements and options, along with some “clinical pearls” that I’ve found to help substantially when managing these conditions.
Case report: Chronic ocular inflammation
A 53-year-old Hispanic male presented with complaints of chronic, bilateral red eyes and a “growth” covering a portion of the cornea OD. He reported a waxing and waning history of lid discomfort, ocular burning and stinging, and persistent hyperemia over the course of approximately 4 years. His systemic history was non-contributory.
Examination revealed cutaneous vascular dilatation along the eyelid margins and facial regions, consistent with erythematotelangiectatic rosacea, including ocular involvement in the form of chronic blepharitis.
There was also evidence of phlyctenular keratoconjunctivitis with extensive stromal neovascularization, warranting surgical intervention. Post-operatively, the patient showed good surface regularity (Figure 1), but continued to suffer from intermittent flares associated with symptomatic blepharoconjunctivitis.
Figure 1 is a close-up of the patient’s eye following surgical intervention with good ocular surface regularity.

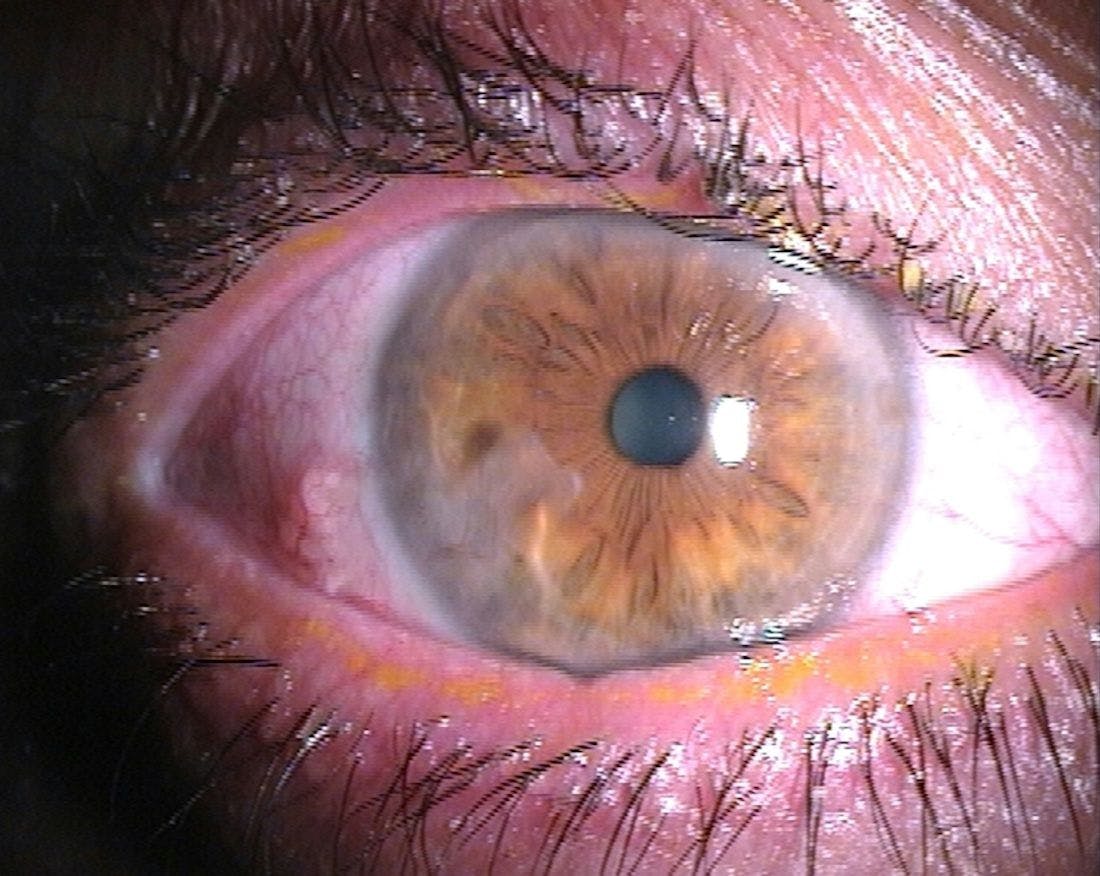
Figure 1: Courtesy of Derek Cunningham OD, FAAO.
Imagine this patient is under your care. How might you maximize his progress and ocular health while minimizing the propensity for continued inflammation and the risk of infection? Read on to learn about my approach to patients like this.
Addressing the acute red eye
Scenarios like the one posed here tend to fall under the broad category of acute red eyes. In such cases, we encounter varying degrees of ocular inflammation within the framework of microbial infection, or in some instances where a microbial infection is suspected, or the risk is elevated due to contributory factors (e.g., trauma, contact lens wear, poor hygiene, etc.).
Some of the more common conditions that ECPs may see include:
- Allergic conjunctivitis
- Viral follicular conjunctivitis
- Microbial keratitis and keratoconjunctivitis
- Traumatic keratitis
- Nonspecific conjunctivitis of recent onset
- Blepharitis and meibomian gland dysfunction (MGD)
- Marginal keratitis (aka “sterile corneal ulcers”)
- Contact lens-associated acute red eye (CLARE)
- Phlyctenular keratoconjunctivitis
- Post-operative status following surgical procedures
In some of these clinical scenarios, the treatment is straightforward and specific. For example, in cases of microbial keratitis, especially those individuals presenting with central or paracentral ulceration presumed to be bacterial in nature, the only acceptable first-line therapy is a robust, broad-spectrum topical antibiotic, used in isolation for 48 to 72 hours.1
Similarly, conjunctivitis that is determined by history and/or classic presenting signs to be allergic or viral in nature should be managed with targeted therapy, whether that be a topical antihistamine/mast cell stabilizer or an antiviral agent (e.g., topical ganciclovir or povidone-iodine therapy, both of which are off-label). However, in many cases where the etiology is unclear, combination agents should be strongly considered.
Are combination agents overused in clinical practice?
One thing that I hear occasionally from colleagues at the podium is that combination agents are overused. However, based on my experience working in a referral center with more than 200 ODs feeding our network, I believe that these agents are, on the contrary, wholly underutilized.
I would say that our most difficult and daunting task as clinicians, especially when we talk about interns and residents, is properly addressing the nonspecific, acute red eye. In community-based care, I’ve learned that when combination agents are used early and correctly, patients do not require a referral in the vast majority of cases because the condition responds very rapidly.
While this might violate the adage, “Never treat without a definitive diagnosis,” these medications that we’re discussing are actually quite safe, and they are designed to cover a broad spectrum of etiologies effectively.
So, while we would always prefer to know exactly what we are treating, the reality is that there are just some situations where the cause is difficult to ascertain with 100% certainty; in these scenarios, the experienced clinician looks toward addressing the presentation itself, which in the acute red eye means controlling inflammation and the risk posed by potential bacterial pathogens.
My philosophy on combination agents
As most of us know, with any significant infection, there will likely be concurrent inflammation, as this is a part of the body’s natural response to pathogenic insult. At a very basic level, this attendant inflammation is actually beneficial since the process serves to “wall off” the infection and allow the immune system to begin attacking the foreign adversary.
Conversely, however, what I’ve learned clinically over the last 20+ years is that with any significant inflammation, we also carry an increased risk of infection. When ocular tissue is compromised by an acute inflammatory stimulus, it becomes less able to defend itself from external stressors such as microbial pathogens.
Many times, these two elements are so pronounced that it becomes difficult to differentiate what precise etiology is at the root of the presentation; hence, the best therapeutic course is to address them both jointly by employing an anti-inflammatory agent and an antimicrobial agent simultaneously.
While there certainly are well-documented risks associated with these agents in specific instances, the experienced clinician should be able to rule out potential contraindications and prescribe these medications with confidence.2
Clinical candidates for combination agents
Let’s discuss some of the aforementioned conditions in greater detail. Here are the top five situations where I’m most often inclined to prescribe a combination agent as my initial form of therapy.
Nonspecific conjunctivitis
Nonspecific conjunctivitis is a vague term used to describe the various acute, red eye presentations with attendant inflammation that may be encountered in a clinical setting. Some sources use this language to characterize eye redness and discharge for which the cause cannot be traced to any specific viral, bacterial, allergic, or toxic entity.3
A systematic review of the literature pertaining to conjunctivitis substantiates this diagnostic dilemma.4 It seems that the key criteria which we often cite for differentiating these etiologies, such as patient symptoms, presence or type of discharge, and duration of the condition prior to presentation, were not specific to any particular class of conjunctivitis.4
And, while it’s long been determined that viruses cause up to 80% of all cases of acute conjunctivitis, the rate of clinical accuracy in diagnosing viral conjunctivitis is less than 50% as compared with laboratory confirmation.5-7
Indeed, a good portion of these cases are actually misdiagnosed and treated as bacterial infections. So clearly, there are “classic” cases of follicular adenoviral conjunctivitis as well as mucopurulent bacterial keratoconjunctivitis, but many times the presentations can be nebulous.
It’s in those atypical cases that we tend to reach empirically for a good, reliable combination agent, with a potent corticosteroid to address the inflammation and discomfort as well as a broad spectrum antibiotic to address any excessive bacterial load on the ocular surface, and prevent any secondary contamination or infection by potential pathogenic bacteria.
I know that some of my colleagues criticize this approach, likening it to effectively saying, “I’m not sure what else to do,” but once again, when we see blatant ocular surface inflammation and we suspect that bacteria may have a role, this is precisely the indication for a combination agent (Figure 2).
Figure 2 highlights idiopathic “acute red eye” in a middle-aged patient. The irregular, peaked pupil is related to prior cataract surgery, not uveitis.

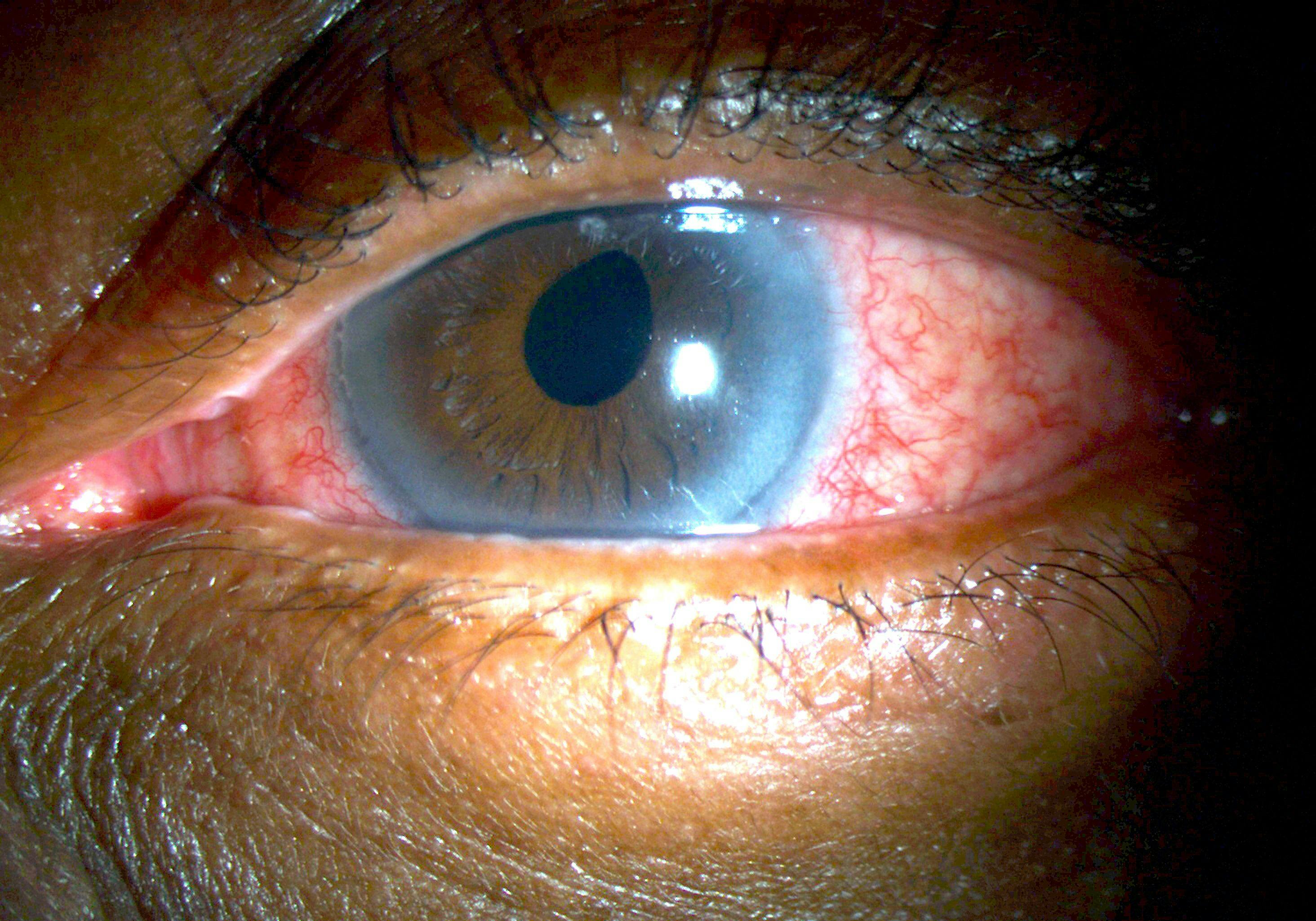
Figure 2: Courtesy of Alan G. Kabat OD, FAAO.
Post-operative status following minor procedures
While the nonspecific red eye is the clinical presentation in which combination agents are most suitable, in our practice, I find that we use these agents most often as prophylactic therapy for in-office lid and ocular surface treatment procedures, e.g., intense pulsed light (IPL) therapy, microblepharoexfoliation, and vectored thermal pulsation for MGD.
An important concept to understand here is that, in any type of treatment for acute eyelid conditions, there is not only a standing bacterial bioload to consider, but also the mechanical treatment itself will induce a fair bit of inflammation.
And so we’ll almost always follow up one of these treatments with a combination drop. We believe that employing this type of therapy for even a week or two dramatically improves patient satisfaction in addition to attaining faster clinical results.
Blepharitis
With regard to blepharitis, many ECPs still prefer to ascribe this condition to a specific category, be it anatomical (e.g., anterior vs. posterior blepharitis) or etiological (e.g., Staphylococcal, seborrheic, or Demodex-associated) in nature (Figures 3a and 3b).
The same principle can be applied to dry eye disease in terms of evaporative vs. aqueous deficient. But if experience has taught us anything, it’s that most of these conditions exist on a continuum, with multiple etiological factors contributing to the manifest clinical presentation.
In our practice, with the exception of truly outstanding cases, we really don’t spend a lot of time educating on the differences between such nuanced conditions. When we’re discussing the treatment of blepharitis, for example, we know that we’re dealing with inflammation and some degree of bacterial overgrowth, so we feel very comfortable initiating induction therapy with a combination agent.
That’s not to say that we’ll treat 100% of cases with these medications in the long term, but the benefit of addressing and reducing the bioburden as well as the inflammation has proven to be the most efficacious initial therapy from both a public health and clinical efficiency standpoint. In our hands, the initial use of a combination agent helps to quiet the eye rapidly and ultimately increases the success of more directed forms of therapy.
Figures 3a and 3b demonstrate pronounced and symptomatic bilateral blepharitis.


Figure 3a: Courtesy of Alan G. Kabat OD, FAAO.


Figure 3b: Courtesy of Alan G. Kabat OD, FAAO.
Acute red eye in a contact lens wearer
The characteristic presentation of a patient with CLARE, also known clinically as marginal keratitis or “sterile” corneal infiltrates, typically consists of a unilateral, swollen, and hyperemic conjunctiva that is most pronounced at the limbal margin.
The cornea may be mildly edematous, with notable areas of small, well-circumscribed infiltrates situated at or near the limbal edge; unlike microbial keratitis, these infiltrates rarely stain extensively with sodium fluorescein (Figures 4a and 4b).
Symptoms of CLARE usually consist of acute onset irritation, ranging from mild to moderate in intensity, as well as photophobia and epiphora. The history is typically positive for overnight contact lens wear, either intentional or otherwise.
Figures 4a and 4b highlight marginal keratitis associated with contact lens abuse. Note the multiple peripheral infiltrates at the temporal limbus (top), which stain very slightly with sodium fluorescein (bottom).

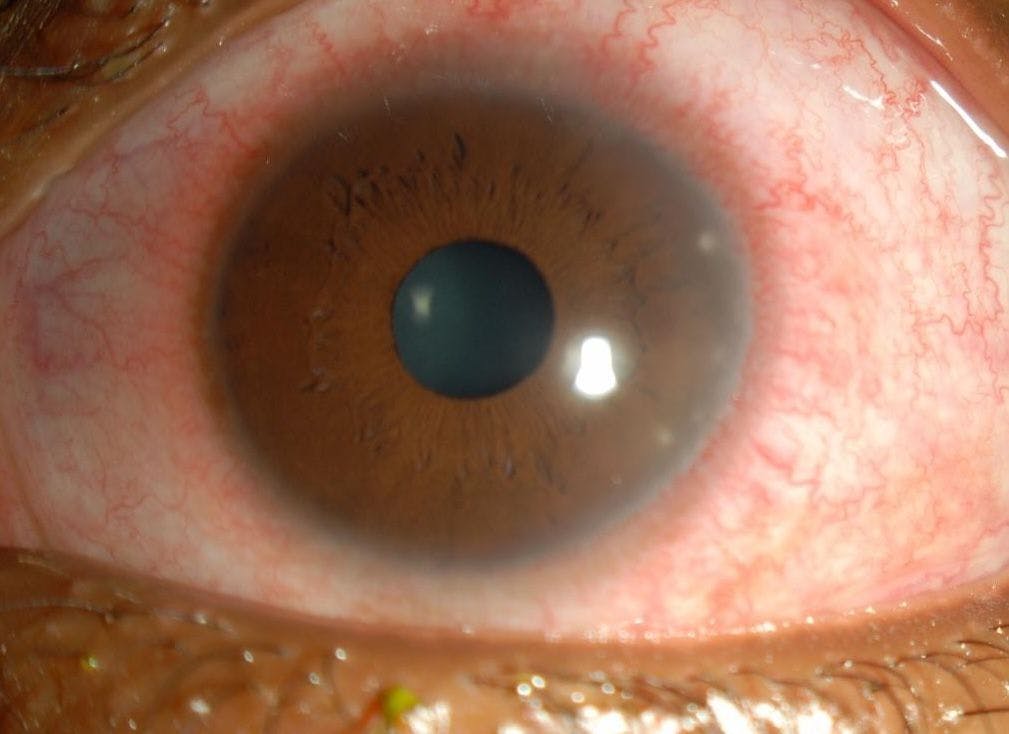
Figure 4a: Courtesy of Alan G. Kabat OD, FAAO.

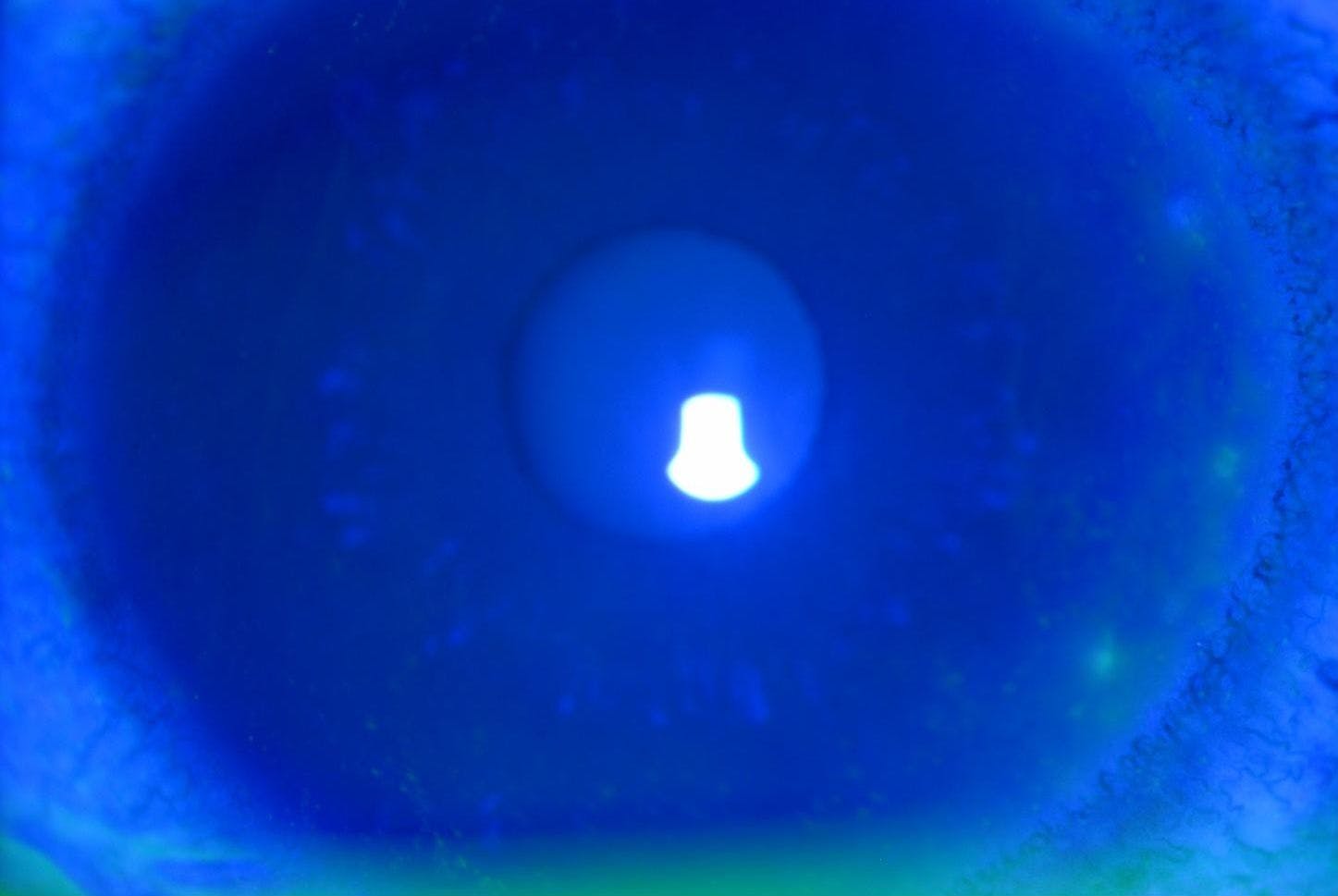
Figure 4b: Courtesy of Alan G. Kabat OD, FAAO.
We recognize that such cases are inflammatory in nature, spurred by hypoxic stress involving the cornea. Additionally, however, the bacteria that colonize contact lens surfaces can also stimulate the inflammatory cascade due to the release of bacterial endotoxins.8-10
Hence, both an agent to suppress inflammation and an antimicrobial to address the bacterial load on the ocular surface are indicated. Therefore the selection of a combination agent in this case is perfectly valid.
It is theoretically far safer than using a corticosteroid alone (since the cornea represents privileged, avascular tissue) and significantly more efficacious than initiating a broad spectrum antibiotic in isolation.
Phlyctenular keratoconjunctivitis
Phlyctenule, whether it involves exclusively the conjunctiva or the cornea as well, represents a nodular inflammation that is the result of a hypersensitivity reaction to foreign antigens (Figure 5).11 Historically, phlyctenule was associated with the tuberculin protein, and was considered to be a strong sign of tuberculosis infection, particularly in malnourished children of lower socioeconomic status.12
Today however, microbial proteins of Staphylococcus aureus are the most common causative antigens in phlyctenular keratoconjunctivitis in the Western world.13 At the most basic level, this condition is representative of a similar pathological cascade; it is the body’s immune system aggressively responding, however inappropriately, to its own tissues.
So the key is tamping down the inflammatory response while also reducing the high bacterial load that provoked the episode, which in the vast majority of cases can be traced to lid margin disease (e.g., blepharitis). Here again, a combination corticosteroid-antibiotic represents the safest and most effective induction therapy.
Figure 5 is a clinical image of phlyctenular keratoconjunctivitis, note the focal, inflammatory lesion straddling the temporal limbus with attendant vasodilation and edema—signifying inflammation.

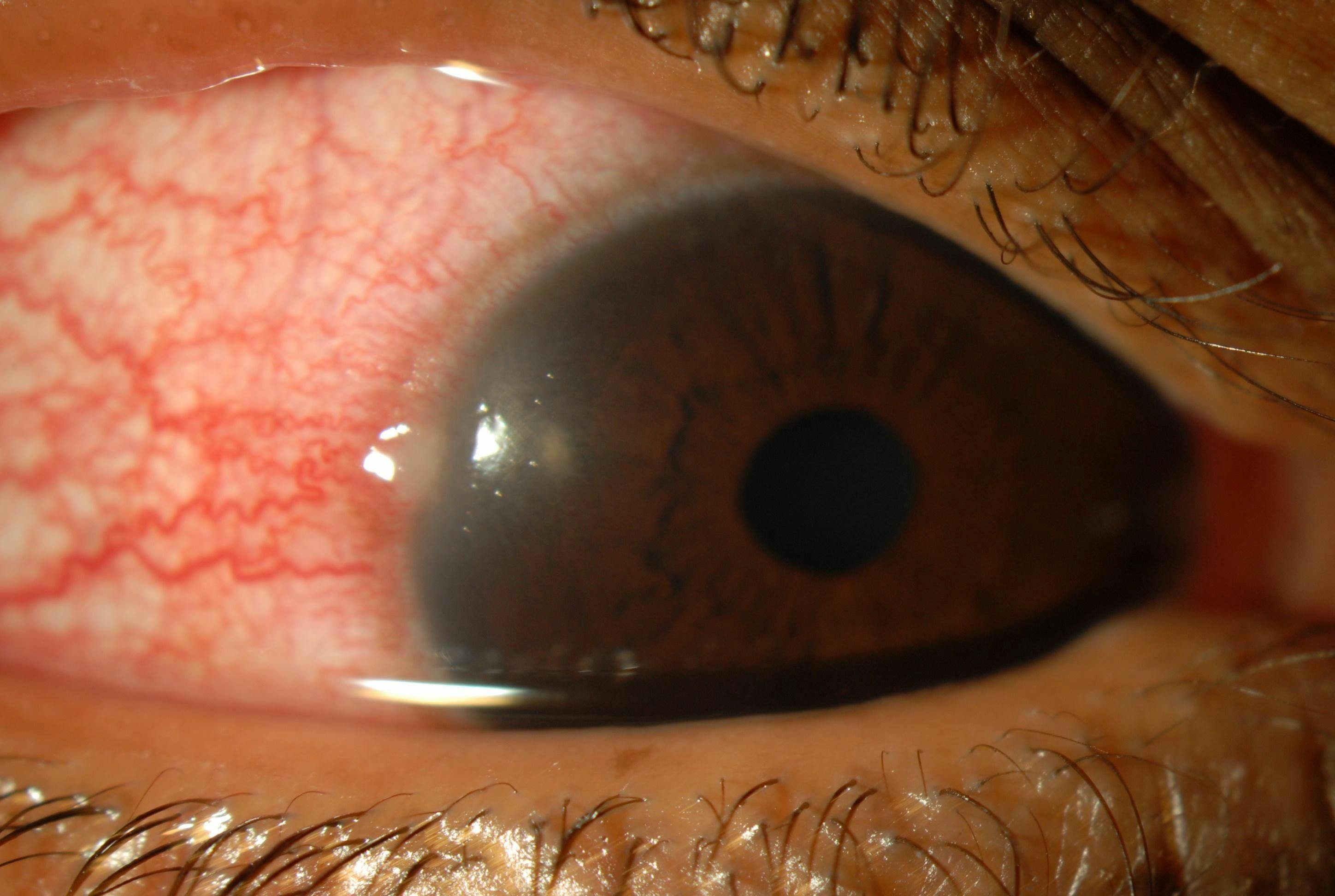
Figure 5: Courtesy of Alan G. Kabat OD, FAAO.
Contraindications, or when to steer clear of combination agents
We’ve discussed several clinical scenarios where a combination steroid/antibiotic is indicated and may be used comfortably as empirical therapy. But certainly, there are a few notable situations in which these agents are contraindicated, and clinicians need to know when such formulations are potentially problematic.
I typically will cite three diagnoses where combination medications should be avoided. The first and most obvious of these is when a dendritic corneal lesion is present or suspected; we never want to use a corticosteroid in the presence of Herpes simplex keratitis, and certainly not without potent antiviral coverage.
But this isn’t even the most significant scenario, in my estimation. Cases in which there is frank, central corneal ulceration indicative of bacterial keratitis warrant treatment with a broad-spectrum antibiotic exclusively for at least 48 to 72 hours, or until some stabilization or improvement is observed. Initiating any corticosteroid in such a scenario poses an unacceptable risk for vision-threatening sequelae.
And finally, the area where I tend to see these combination agents inappropriately utilized, often to excess, is in the treatment of vague, watery red eyes by general practitioners. Upon proper examination, many of these turn out to be classic follicular adenoviral conjunctivitis or even seasonal allergic conjunctivitis, and quite frankly we have far better medications with which to manage these conditions.
In the case of allergic patients, I’ve even seen some individuals who respond negatively to the tobramycin component in some of these agents, and their condition actually worsens (Figure 6).
Figure 6 shows a patient who returned 3 days after being prescribed a combination drop containing 0.1% dexamethasone with 0.3% tobramycin for a presumed bacterial conjunctivitis. He reported severe itching and burning, increased watery discharge, and more pronounced swelling and redness, all indicative of a contact allergic reaction.


Figure 6: Courtesy of Alan G. Kabat OD, FAAO.
Selecting and prescribing combination drug therapies
According to the US Food and Drug Administration (FDA)-approved prescribing information for all medications in this category, topical ophthalmic pharmaceutical agents containing both corticosteroids and antibiotics should be employed specifically “...for steroid-responsive inflammatory ocular conditions for which a corticosteroid is indicated and where superficial bacterial ocular infection or a risk of bacterial ocular infection exists.”14-17
At present, there are a number of combination agents available in the United States. Most of these are generic products, combining corticosteroids such as prednisolone sodium phosphate or dexamethasone with aminoglycoside (e.g. neomycin, tobramycin) or sulfonamide antibiotics.
Over the last 20 years, the most commonly prescribed agents in this class (in order of FDA approval) include:
- Maxitrol (0.1% dexamethasone + neomycin [3.5mg/mL] + polymyxin B [10,000 units/mL])
- TobraDex (0.1% dexamethasone + 0.3% tobramycin)
- Zylet (0.5% loteprednol etabonate + 0.3% tobramycin)
- TobraDex ST (0.05% dexamethasone + 0.3% tobramycin).
Table 1 lists currently commercially available, FDA-approved combination corticosteroid/antibiotic agents.

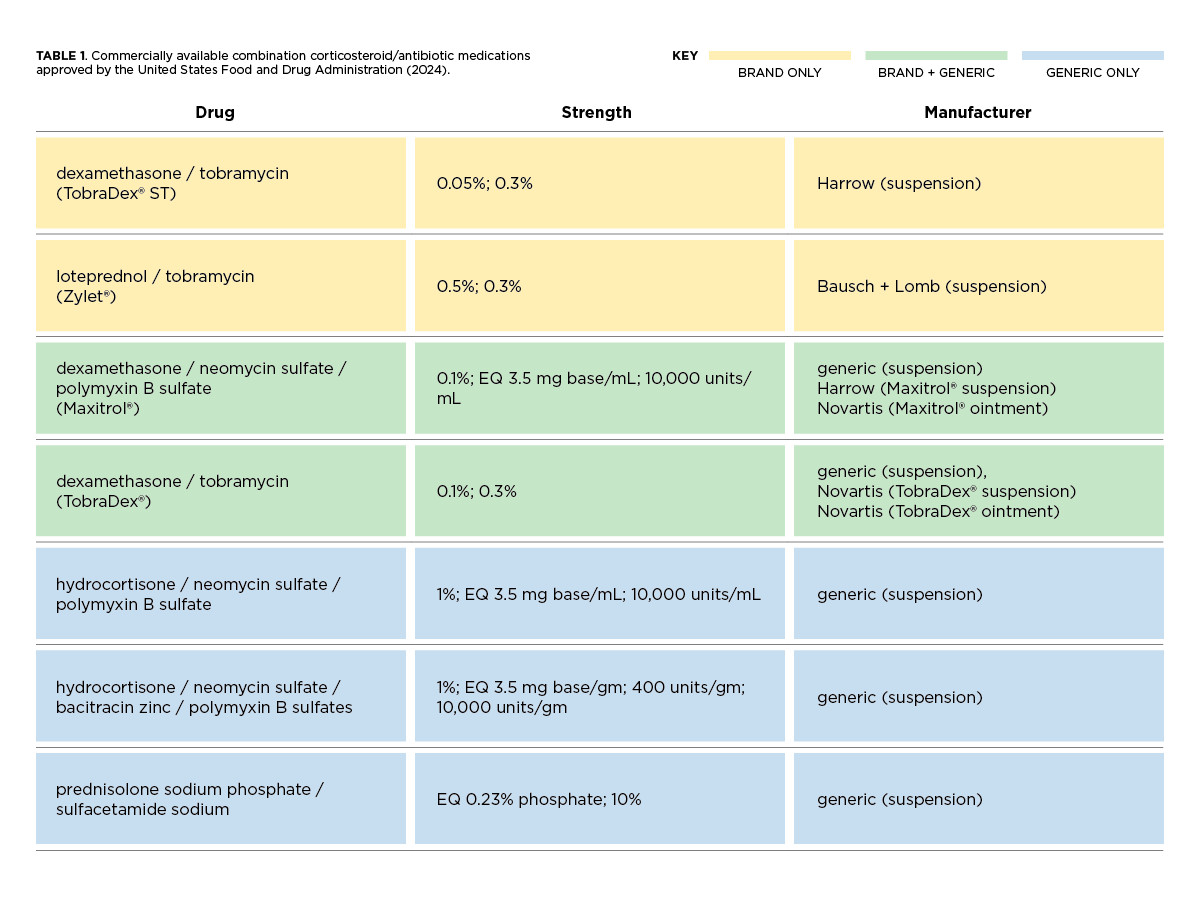
Table 1: Courtesy of the authors.
Combination medications have a unique place in eyecare. By combining a corticosteroid with an antibiotic, this group of drugs imparts both anti-inflammatory and anti-infective properties, making it the ideal choice for patients with inflammatory ocular disorders that may also involve (or be at risk for) a bacterial component.
Clinically, we tend to use these combination agents for specific conditions, including such entities as acute blepharoconjunctivitis, contact lens-associated acute red eye, marginal keratitis, superficial corneal trauma, and shield ulcers (associated with vernal or atopic keratoconjunctivitis).
And, right or wrong, many practitioners also tend to employ these agents for the “idiopathic” red eye—those presentations that do not fit neatly into any specific diagnosis, but seem to require both anti-inflammatory therapy along with antimicrobial prophylaxis.
Hence, combination medications are often our “go to” drugs in severe or bewildering cases. We rely on these medications to provide rapid relief of symptoms and initiate the resolution of inflammation in a short period of time.
Branded or generic combination agents?
The more we are put in pressure situations as clinicians, the easier it becomes to “see the cracks” as it were in any therapeutic selection. With regard to generic ophthalmic medications, the FDA does not require clinical trials to demonstrate efficacy, as their approval is based upon the results of their branded counterparts.
Generics, while chemically similar, may have a variety of manufacturers and slight variations in formulation that can influence their tissue absorption and pharmacodynamics, sometimes significantly.
So while 3rd parties have had tremendous influence on the medications that patients ultimately receive, we know from personal clinical experience that these options have certain limitations and often a less favorable side effect profile.
And I can say with confidence that, all other things being equal, I would never prescribe a generic because of the inherent lack of safety and efficacy data.

As far as clinical comparisons, there are only a few head-to-head trials on which to base our decisions. In a multicenter, randomized, investigator-masked study, researchers found that loteprednol etabonate 0.5% / tobramycin 0.3% (Zylet) was non-inferior to dexamethasone 0.1% / tobramycin 0.3% (TobraDex) in the treatment of ocular inflammation associated with blepharokeratoconjunctivitis.18
Moreover, subjects who received the dexamethasone/tobramycin compound experienced a greater mean increase in intraocular pressure (IOP) than their counterparts, with twice as many individuals experiencing an IOP elevation of 5 to 10mmHg over the course of 15 days.
The rate of treatment-emergent adverse events was also more than double in the dexamethasone/tobramycin group as compared to the loteprednol etabonate/tobramycin group (6.5% vs. 2.9%).18
Dosage and duration of combination agents
Obviously, any time we’re utilizing a topical corticosteroid to treat inflammation, the dosing frequency and the duration of treatment will be dependent on the degree to which the ocular tissues are inflamed, as well as the patient’s response to therapy.
Ideally, my strategy is to initiate treatment early and aggressively so as to minimize inflammatory sequelae. The biggest mistake that I see in terms of these combination drugs is that doctors often fail to use them long enough or frequently enough.
Just considering the antimicrobial element, we want to achieve bactericidal levels as quickly as possible. When we’re discussing a topical aminoglycoside like tobramycin, that means dosing at least every 6 hours (QID).
That same premise also holds true for inflammation. In the simplest of terms, if you’re too timid with these medications, you’ll run the risk of a smoldering infection as well as persistent or rebound inflammation.
Patients should also be advised to use these medications for a full course of therapy, which in most instances should be at least 10 days. That said, any therapy needs to be monitored for responsiveness, potential adverse reactions, and other complications that may prompt us to adjust our initial therapeutic strategy.

Conclusion
Combination agents containing anti-inflammatory corticosteroids and broad-spectrum antibiotic agents have a distinct place in the management of acute, “red eye” presentations. While the guidelines are clear regarding when and how these medications should be utilized, many practitioners remain hesitant to prescribe them, or use them very sparingly.
This hesitation seems most often to be rooted in fear of exacerbating a handful of relatively uncommon ocular conditions, and/or misconceptions about the safety of this class of medications. Nevertheless, if we are diligent in our diagnostic evaluation and understand the specific indications, contraindications, and limitations associated with these agents, we can confidently utilize them with near impunity.
The potential benefits of employing combination therapy far exceed the downside, provided we: (1) always use our best clinical acumen; (2) recognize those conditions that are specifically at-risk; and (3) always provide appropriate monitoring and follow-up care.


