




A macular hole (MH) is a full-thickness defect in the fovea, resulting in decreased visual acuity or metamorphopsia. Gass first classified this entity in a system still widely utilized clinically in its management today.
Before optical coherence tomography (OCT) imaging, Gass theorized that MH formed due to anterior-to-posterior vitreoretinal traction and tangential retinal traction.1
Understanding macular hole classification
In the Gass classification system, MHs were described in the following manner:
- Stage 1: Represents partial thickness foveal disruptions.
- Stage 1a: Characterized by foveolar detachment with loss of the foveal contour appearing clinically as a lipofuscin-colored spot 100 to 200μm in diameter.
- Stage 1b: Characterized by foveal detachment appearing clinically as a lipofuscin-colored ring 200 to 350μm in diameter.
- Stage 2: A full-thickness retinal defect <400μm in diameter with vitreomacular traction (VMT).
- Stage 3: A full-thickness retinal defect ≥400μm in diameter with VMT.
- Stage 4: A Stage 3 hole that has progressed to involve complete posterior vitreous detachment (PVD) with the appearance of a Weiss ring.1
Figure 1 demonstrates a dissecting microscope image of a macular hole.

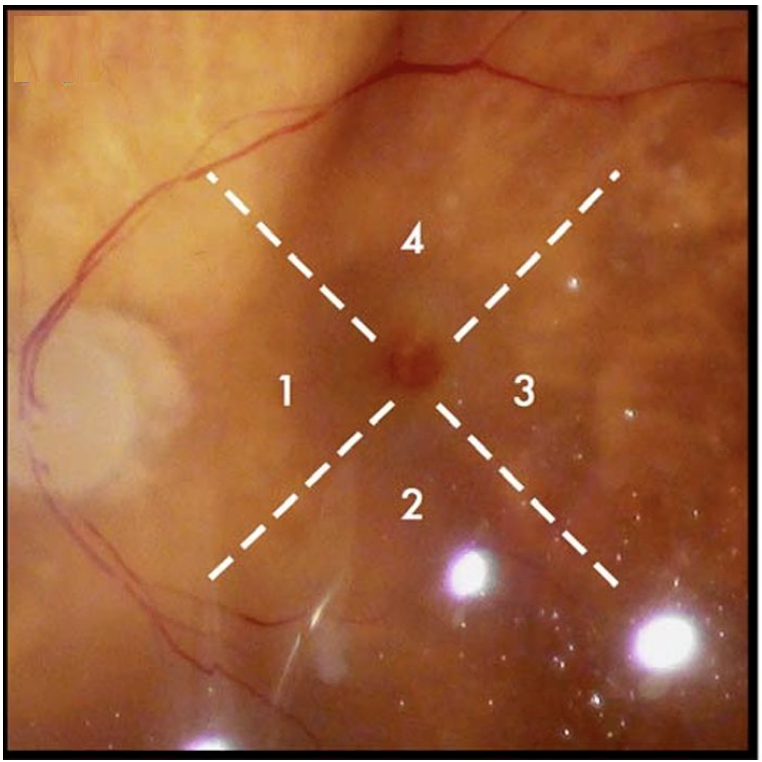
Figure 1: Courtesy of David Almeida, MD.
In Figure 2, a low magnification scanning microscope image of the specimen was captured after treatment with a Tano scratcher showing light pressure applied to the area at point 1, medium pressure applied to the area at point 2, and heavy pressure applied to the area at point 3, which shows disruption of the internal limiting membrane and exposure of the nerve fiber layer at point 4. Note some of the cellular tissue has fallen into the hole.

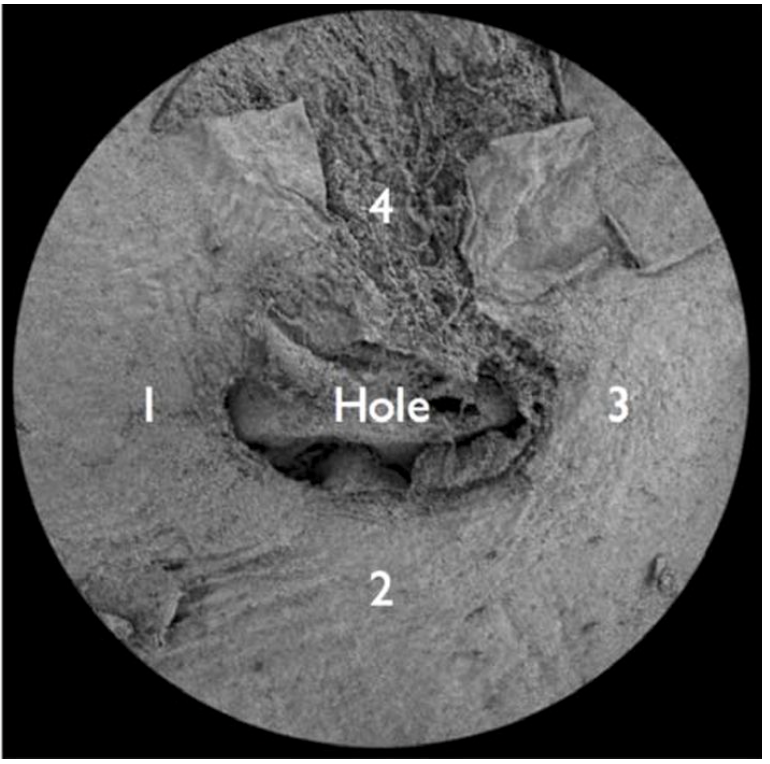
Figure 2: Courtesy of David Almeida, MD, and Eric K Chin, MD.
Staging MHs with OCT characteristics
With the advent and study of OCT, an international classification of vitreomacular adhesion (VMA), VMT, and MH based on OCT characteristics has been more recently published.2
In this classification system, MH is defined as a full-thickness anatomic defect in the fovea with interruption of all layers of the neurosensory retina from the internal limiting membrane (ILM) to the retinal pigment epithelium (RPE). These defects are then characterized secondarily based on size, the presence or absence of VMT, and whether the etiology is primary (i.e., idiopathic) or secondary.
In Figure 3, spectral-domain optical coherence tomography (SD-OCT) reveals a typical full-thickness macular with the absence of posterior detachment.

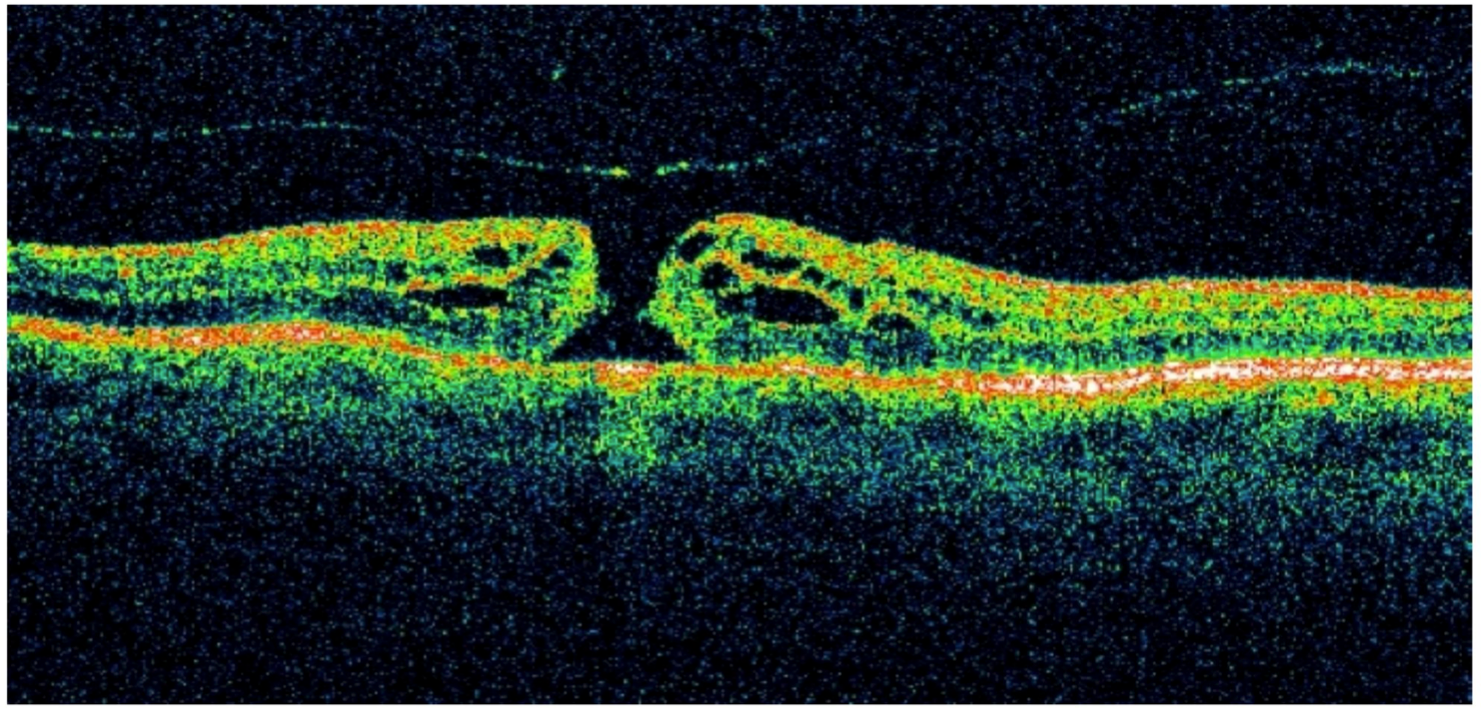
Figure 3: Courtesy of David Almeida, MD.
Using studies that published rates of successful hole closure via intravitreal ocriplasmin or pars plana vitrectomy (PPV), small MHs are <250μm, medium MHs are 250 to 400μm, and large MHs are >400μm based on minimum hole diameter as measured by OCT.
In Figure 4, SD-OCT shows a small full-thickness macular hole with perifoveal cystic changes.

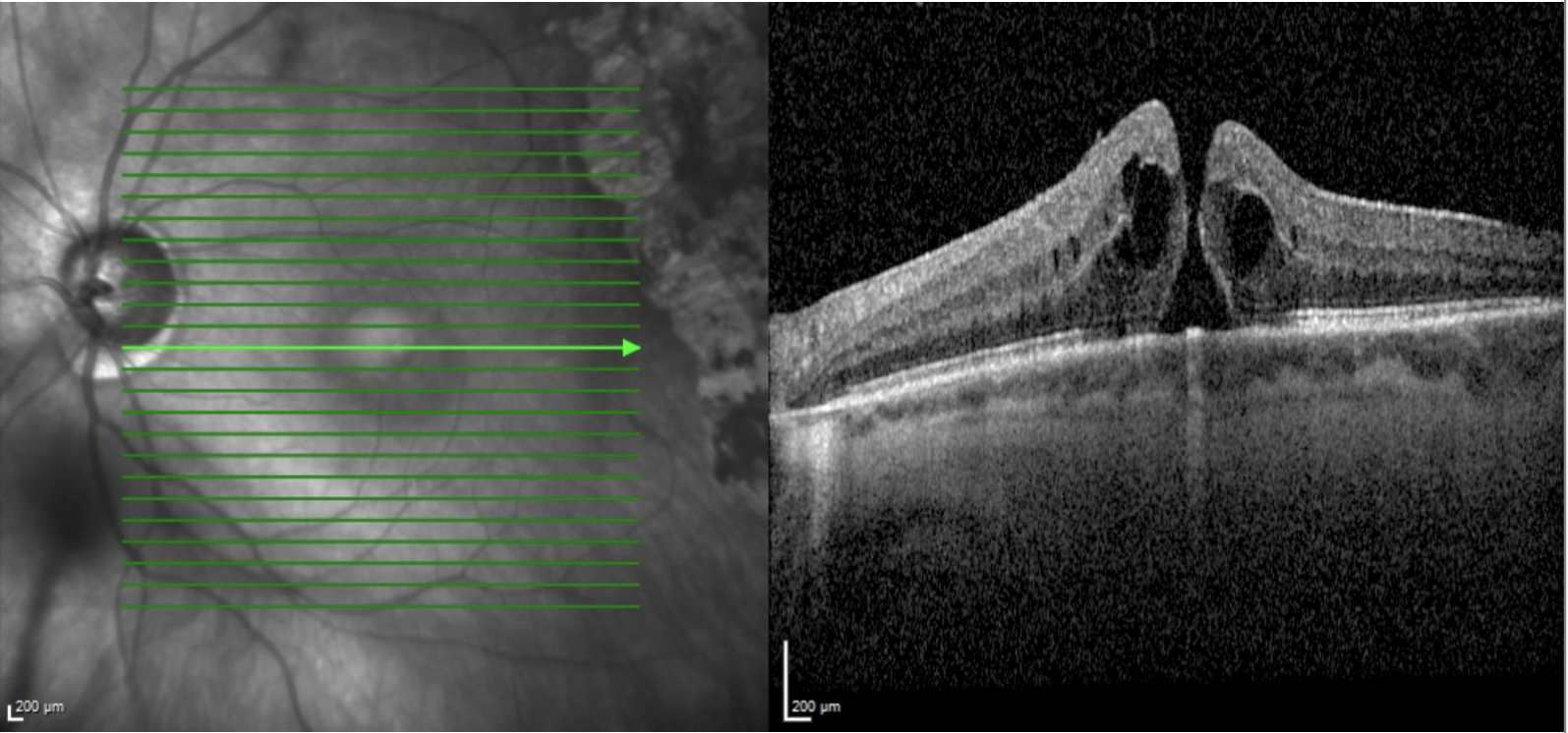
Figure 4: Courtesy of David Almeida, MD.
Small holes generally have high closure rates via PPV and were sometimes responsive to intravitreal ocriplasmin (i.e., Jetrea, when it was previously available, 2012 to 2020). Medium holes also have high closure rates via PPV with or without ILM peeling, and select cases may have responded to intravitreal ocriplasmin.2
However, large holes generally do not respond to ocriplasmin. Examples of secondary causes of MH include blunt or surgical trauma, high myopia, macular schisis, macular telangiectasia type 2, exudative (wet) age-related macular degeneration (AMD), retinal macroaneurysm, and lightning strike.
Decision-making in managing clinically significant MH is often determined by size, chronicity, and pre-operative best-corrected visual acuity (BCVA). This article will review the surgical management of MH.
Macular hole surgical management techniques
Pars plana vitrectomy
Spontaneous closure of full-thickness MH is rare and was initially thought to be an “incurable” disease.3 PPV was first described in a prospective study by Kelly et al. in 1991.3 Their pilot study described outcomes of PPV, removal of adherent VMT (for Gass Stage 2 holes), ERM removal, and complete air-fluid exchange.
In total, 30 of 52 eyes (58%) achieved hole closure with this technique, with most eyes having an improvement in BCVA of two lines or better. Two patients had iatrogenic worsening of MH during attempted aspiration of serous fluid above the macula, resulting in RPE mottling.3 They proposed that relieving vitreous traction on the macula with PVD induction is critical in allowing the hole to close.
A meta-analysis of randomized controlled trials comparing PPV to observation showed, on average, a 1.5 Snellen line (-0.16 logMAR) improvement in BCVA at 6 to 12 months and an odds ratio of 31.4 for closure at 6 to 12 months.4 However, these trials utilized techniques and instrumentation such as larger gauge cannulas that may need to be updated and may not apply to current-day management.
The development of smaller vitrectomy cannulas has been associated with improved surgical outcomes lower rates of complications including iatrogenic retinal breaks, shorter operating times, and lower post-operative intraocular pressure.5
An extensive retrospective review of patients who underwent MH repair with small gauge (23- or 25-gauge) PPV only showed that 13 of 392 (3.3%) cases had at least one hole recurrence, slightly lower than reported rates in older studies using 20-gauge cannulas.4,6
Possible contributing factors to improved outcomes with small gauge cannulas include decreased rates of post-operative inflammation and cystoid macular edema (CME) and improved ILM peeling techniques and instrumentation.6
Internal limiting membrane peeling
Over time, various techniques have been implemented to augment PPV. One of the earliest advances in the surgical management of MH is ILM peeling, first described by Eckhardt et al. in 1997.7
Following standard PPV and PVD induction, intraocular forceps are used to grasp the ILM with or without the creation of a flap tear and peeled in a circular area over the fovea in a fashion similar to that of the capsulorhexis during cataract surgery. Proposed hypotheses for the benefit of ILM peeling include reduced rates of ERM formation via removal of the scaffold for cellular proliferation, thus reducing the risk of tangential forces that may lead to hole opening.
Another hypothesis is that the mechanical trauma of ILM peeling may induce local cytokine release, promoting glial cell proliferation, which may assist with hole closure.8 Various studies have suggested that ILM peeling reduces the risk of hole reopening.
One meta-analysis of 5,480 MH surgeries across 50 publications found that 125 of 1,756 (7.12%) eyes that underwent PPV without ILM peeling had recurrence, while 44 of 3,724 (1.18%) with ILM peeling had recurrence. Notably, however, there was no statistically significant difference in the final BCVA between the two groups, which may be due to reoperation on reopened MH.8
Advances in ILM technique since the procedure was first described include staining with indocyanine green (ICG), triamcinolone acetate, and brilliant blue G (BBG) and improvements in instrumentation (e.g., disposable small gauge ILM forceps).
Performing gas or oil tamponade with face-down positioning
Most surgeons perform an air-fluid exchange after PPV with or without ILM peeling to re-approximate the edges of the MH retinal defect via mechanical tamponade. The surgeon may elect to instill non-expansile gas (SF6 or C3F8) tamponade or, less commonly, silicone oil (SO) for larger MH or for patients who need to travel to higher altitudes in the early post-operative course.
The spectral-domain optical coherence tomography in Figure 5 shows a repaired macular hole after internal limiting membrane peeling with intraocular gas tamponade. Note the inner retinal irregularities post-macular surgery.

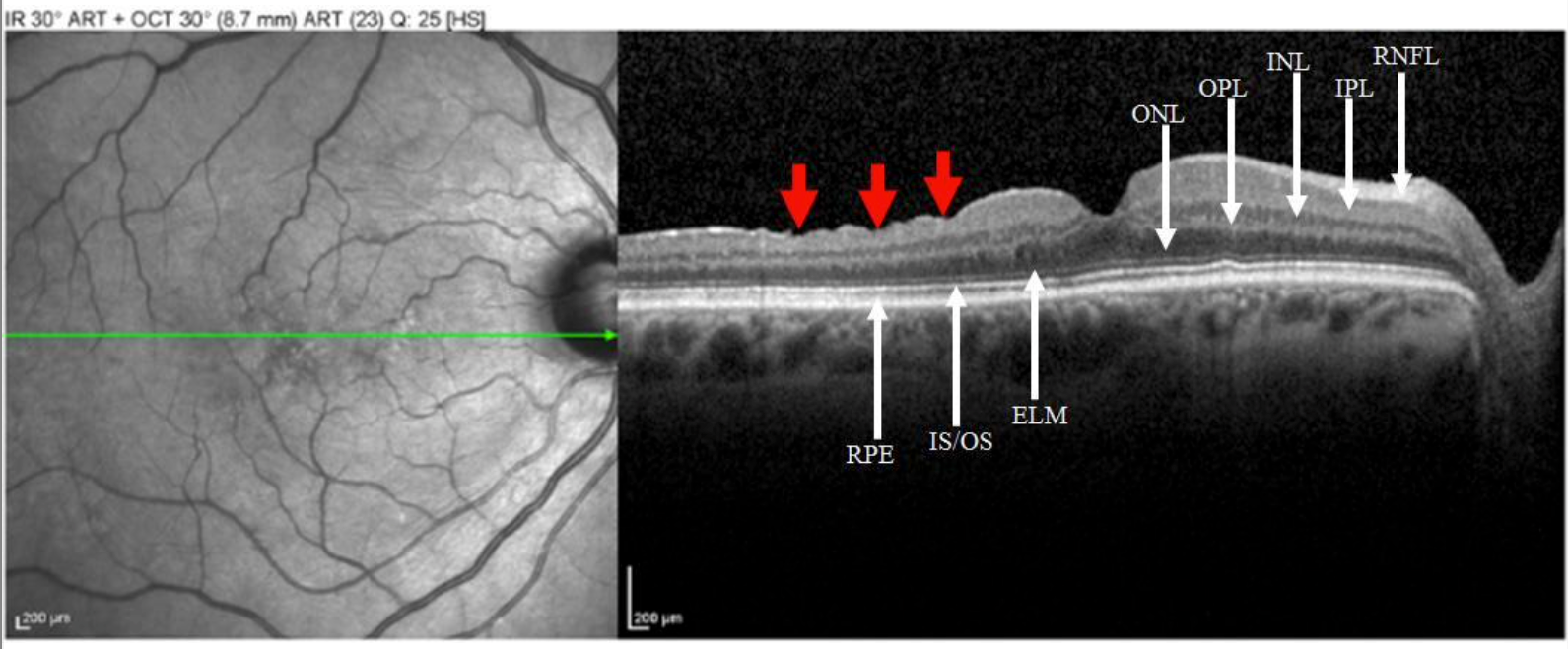
Figure 5: Courtesy of David Almeida, MD.
The most significant difference between these agents is the duration of face-down posturing or the necessity of posturing. One retrospective comparative study found significantly higher reoperation rates in patients with SO injection than C3F8 gas.9 Given lower initial closure rates and the necessity of subsequent SO removal, few surgeons opt for this method of tamponade.
Face-down positioning is often challenging for patients, and compliance may be an issue for those with other medical co-morbidities. A meta-analysis of publications comparing tamponade agents found no statistically significant difference in anatomic closure rates.10 Also, there was no definitive evidence that posturing correlates to improved closure rates.
Other studies have also found no significant difference in MH reopening with gas versus air tamponade. Thus, the duration of tamponade and exact instructions for "face-down" positioning after surgery remains controversial.11
Inverted ILM flap technique
Since the development of inverted internal ILM peeling, other techniques have been devised and studied, all to cover the retinal defect. In the inverted ILM flap technique, rather than completely removing the ILM, intraocular forceps are used to harvest a circular rim of ILM tissue, which is left attached to the margins of the MH.
The remaining ILM is then rolled over the hole so that its anterior face, which initially faces the vitreous, is pressed onto bare RPE. This modification to the standard ILM peel aims to reduce the “flat-open” MH recurrence rate, in which bare RPE is left facing the vitreous cavity, by promoting the proliferation and migration of glial cells over the hole.12
First described in a small randomized clinical trial by Michalewska et al., they compared a group of 51 eyes to standard 3-port PPV with ILM peel and air injection to 50 eyes with PPV with attempted inverted ILM flap.12 In total, 7 of the 50 eyes converted to ILM peel intraoperatively. Of the remaining 43 eyes, none developed hole recurrence at a follow-up of up to 12 months. The inverted ILM flap group also had better BCVA than the ILM peel group (logMAR 0.28 vs. logMAR 0.17, P = 0.001).
Various modifications to the ILM flap have been described, including the temporal inverted ILM flap, large semicircular inverted ILM flap, C-shaped temporal inverted ILM flap, pedicle ILM transposition flap, cabbage leaf inverted ILM flap, floating ILM flap, free ILM flap, and multiple free ILM flap.13 These techniques aim to cover large MH and provide a scaffold for glial proliferation.
Lens capsular flap transplantation
The lens capsular flap transplantation (LCFT) technique was developed and intended for application for large refractory MH. Autologous anterior lens capsular tissue from a capsulorhexis performed during simultaneous cataract surgery or allogenic tissue from a donor undergoing cataract surgery on the same day is harvested in balanced salt solution (BSS) and stained with ICG or BBG.
Following standard 3-port PPV with ERM and ILM peeling and air-fluid exchange, the lens capsular tissue is introduced into the vitreous cavity, which is then cut to the appropriate size via a vitreous cutter. The flap is then placed over the MH. This technique has also been combined with autologous blood application to act as an adhesive for the flap.14
In the most extensive published study, the closure rate for LCFT in refractory MH with average diameters ranging from 863 to 1452μm was 96% (48/50).14 Median BCVA went from logMAR 1.78 to 1.00. As of the writing of this article, no prospective studies are comparing LCFT to traditional techniques.
The main disadvantage of this technique is the requirement of combined cataract extraction surgery in phakic patients or a donor undergoing cataract surgery on the same day for patients with aphakia or clear crystalline lenses.
Autologous neurosensory retinal transplantation
Similar in concept to ILM free flaps and lens capsular flaps, autologous neurosensory retinal transplant aims to treat refractory macular holes by providing a scaffold for glial cell proliferation.
Grewal et al. first described this technique in managing a large MH with retinal detachment (RD) secondary to high myopia.15 Following standard PPV, PVD induction, and ILM or ERM peeling, a transplant harvest site in the nearby peripheral retina (outside of the macula) is selected, and its boundaries are marked and barricaded with endolaser and endocautery.
A circular flap of approximately 2 disc diameters is meticulously excised in a bimanual fashion with forceps and intraocular scissors. This step may also be facilitated with the formation of a bleb via subretinal BSS injection. The free flap is then migrated over the MH and flattened over the bare RPE with perfluoro-n-octane (PFO) liquid and gentle manipulation. PFO-silicone oil or PFO-gas exchange is then performed, and the patient is instructed to position face down.
In an anatomical follow-up study of 10 patients who underwent this procedure, autologous neurosensory retinal flap was shown to integrate well with the surrounding native retina, and there was restoration of the foveal ellipsoid zone (EZ) in nine of these patients with statistically significant improvement in post-operative BCVA.16
Neurosensory retinal transplantation may be most advantageous in patients with high myopia due to the fragility of ILM tissue, poor ILM staining, and the presence of concomitant staphyloma.
Conclusion
Today, overall success rates of MH closure are high, up to over 90%. However, several factors may predispose some patients to failure or reopening, such as MH size, more significant disease duration, associated chorioretinal atrophy, retinoschisis, cystoid macular edema, and MH secondary to high myopia and trauma.
Although there is no consensus on the most productive approach, several techniques now exist for managing refractory MH or secondary MH with excellent anatomic and functional visual outcomes.


