


Welcome back to Ready, Set, Retina. In this episode, Daniel Epshtein, OD, FAAO, sits down with Carolyn Majcher, OD, FAAO, to review a case report on a patient with geographic atrophy (GA) that highlights how eyecare practitioners (ECPs) can utilize multimodal imaging for early detection and predicting the progression of the disease.
Each year in the US, an estimated 160,000 new cases of GA are diagnosed, adding to the 1 million currently diagnosed GA patients.1 Primary care optometrists are the predominant entry point for patients with this advanced form of age-related macular degeneration (AMD). Therefore, it is paramount that ODs utilize all of the tools at their disposal to proactively detect the earlier stages of geographic atrophy.2
Through this case study, Dr. Majcher emphasizes the importance of employing multimodal imaging, especially optical coherence tomography (OCT), to detect biomarkers that are fundamental in diagnosing GA.
Geographic atrophy case report
A 70-year-old white male presents with a history of dry AMD in both eyes, with OCT imaging showing extrafoveal, non-center-involved geographic atrophy. The best-corrected vision was 20/20 in the right eye and 20/25 in the left eye—demonstrating that visual acuity can be quite good, despite the presence of advanced AMD.
The patient is non-compliant with AREDS2 supplementation. He had undergone cataract surgery in both eyes. He is a nonsmoker, and his past medical history is remarkable for hypertension, high cholesterol, sinus bradycardia, and heart disease—resulting in a left coronary artery stent. It should be noted that these conditions are not uncommon in AMD patients.
At the time of assessment, he was taking a range of medications, including:
- Lisinopril
- Atorvastatin
- Clopidogrel
- Hydroxyzine
- Aspirin (81mg)
- Multivitamin
- Nitroglycerin PRN
GA biomarkers on multimodal imaging
CFP diagnostic biomarkers
In the initial examination, OCT and color fundus photography (CFP) demonstrated several features that serve as high-risk biomarkers for progression to advanced macular degeneration or, more specifically, GA.
Figure 1 demonstrates baseline color fundus photography of the left eye, which eventually progressed to extrafoveal multifocal GA.

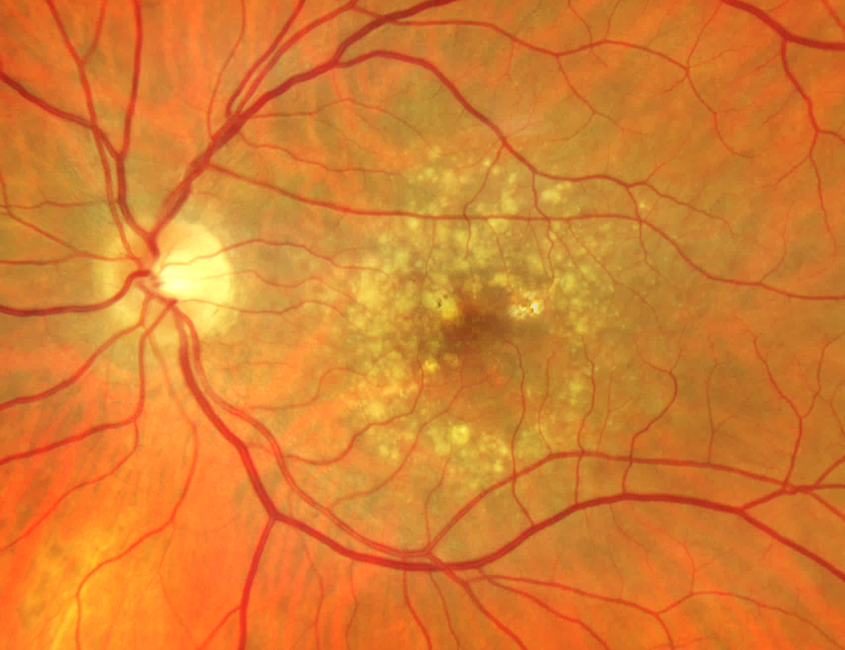
Figure 1: Courtesy of Carolyn Majcher, OD, FAAO.
Color fundus photography revealed:
- Hyperpigmentation overlying a large drusen.
- Pigmentary changes are a documented risk factor for progression to advanced macular degeneration.
- Refractile-type drusen, specific for GA progression.
- Also visible through ophthalmoscopy.
- Increased visibility of the choroidal vasculature corresponding to an area of impending GA.
OCT diagnostic biomarkers
Figure 2 shows intraretinal hyperreflective foci (HRF) indicating anterior migration of retinal pigment epithelium (RPE) cells, loss of the ellipsoid zone, and sub-RPE plaque. Of note, hyperreflective crystalline deposits are also a biomarker of GA progression on OCT.

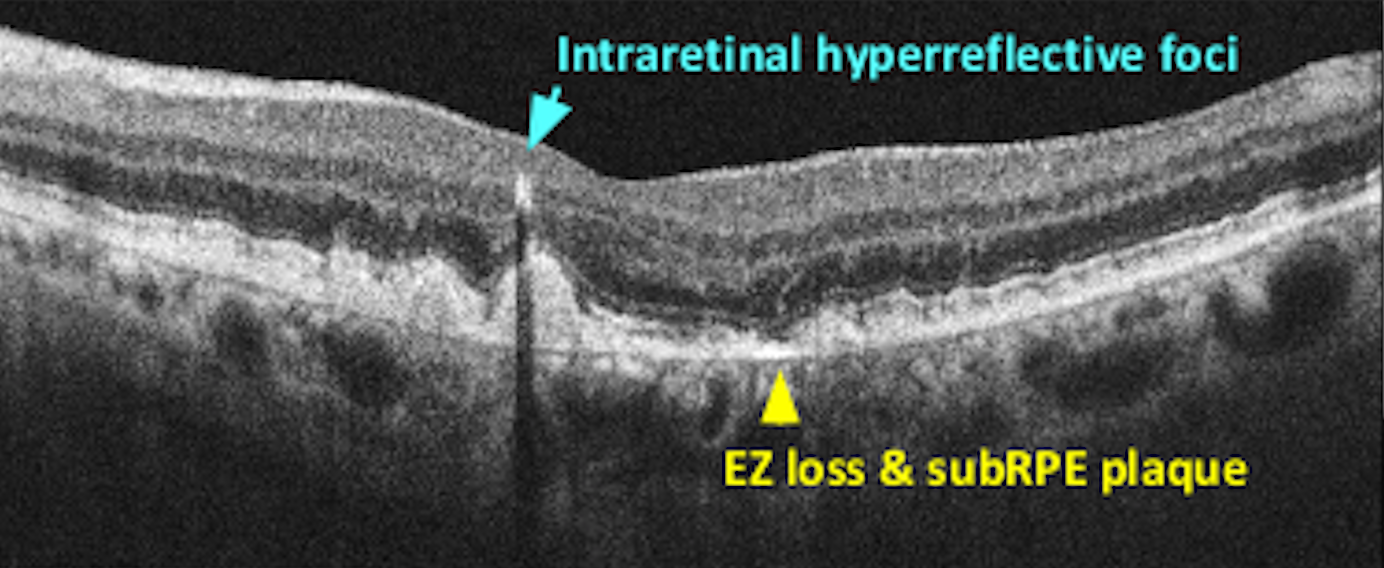
Figure 2: Courtesy of Carolyn Majcher, OD, FAAO.
Figure 3 highlights reticular pseudodrusen (also referred to as subretinal drusenoid deposits [SDD] because they are located between the photoreceptors of the retina and the RPE). As this type of drusen indicates a particularly high risk for GA development, it is valuable to subtype drusen using OCT.3

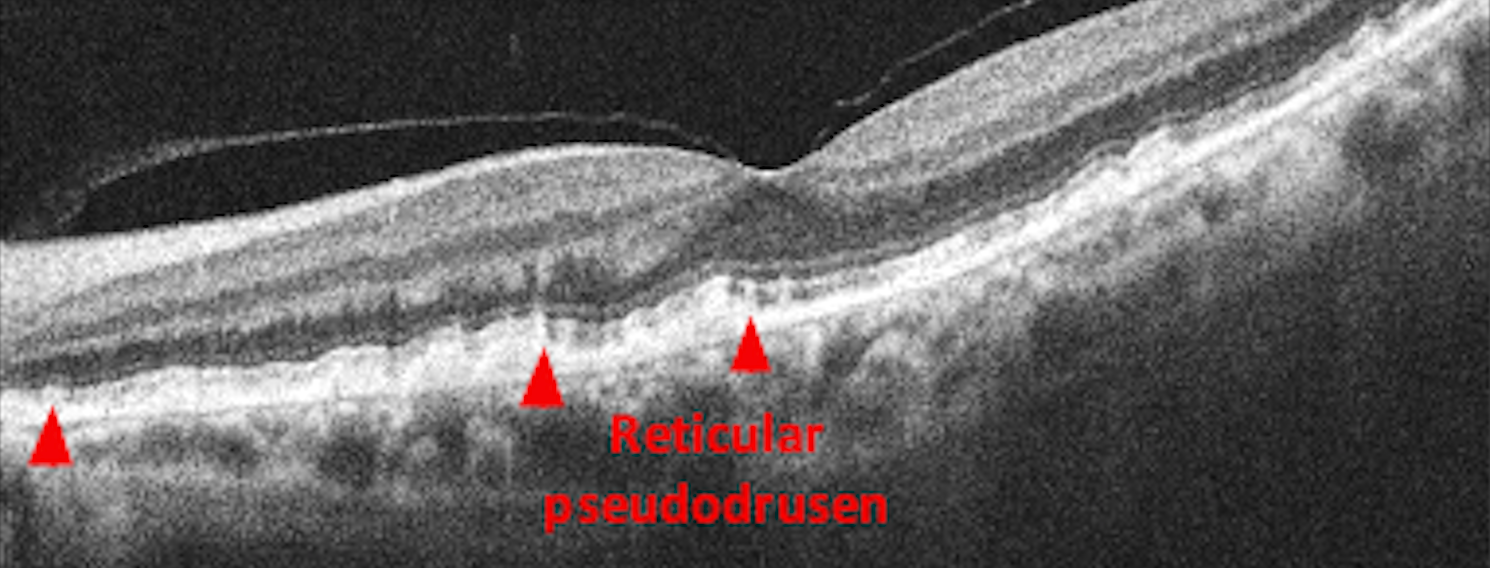
Figure 3: Courtesy of Carolyn Majcher, OD, FAAO.
Key biomarkers of GA progression include:
- Choroidal hypertransmission signaling nascent geographic atrophy lesion as the RPE begins to attenuate.
- Hyporeflective wedges bordering the zone of nascent GA.
- Subsidence of the inner plexiform layer (IPL), forming a V-shaped configuration.
In Figure 4, OCT shows hyporeflective wedges (blue) and “V”-shaped IPL subsidence (pink) indicating impending GA.

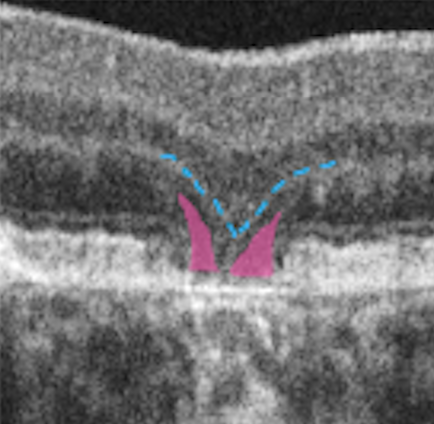
Figure 4: Courtesy of Carolyn Majcher, OD, FAAO.
GA patient progression
Over the course of 3 years, the patient went on to develop extrafoveal multifocal GA bilaterally. Drusen collapse was noted in an area of initial large soft drusen and hyperreflective foci. Regression of drusen or drusenoid pigment epithelial detachments (PEDs) represents one mechanism through which GA can form.4
Areas that displayed sub-RPE hyperreflective plaques and loss of the ellipsoid zone also began to develop early GA. In the adjacent space, vertical columns of choroidal hypertransmission predict another zone of oncoming GA.
Using multimodal imaging to predict GA
Multimodal imaging studies are crucial to not only help with early GA detection, but to predict the rate and breadth of lesion expansion.
Near-infrared reflectance imaging
Dr. Majcher recognizes OCT-generated near-infrared reflectance (NIR) imaging as a highly underutilized tool that is extremely effective in the detection and monitoring of GA over time. With this technology, which is included with the majority of OCT units, areas of geographic atrophy appear hyperreflective.
In Figure 5, we see the progression at baseline, 1.5 years, and 3 years using NIR.

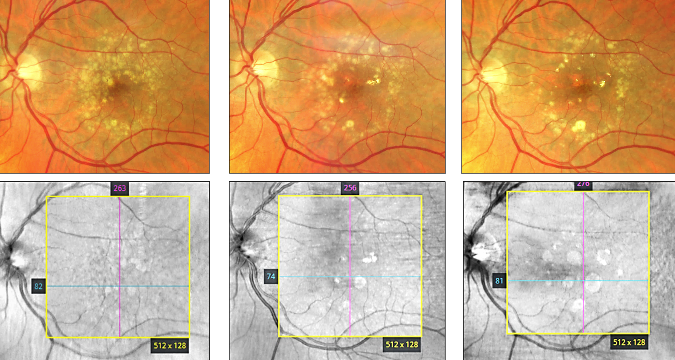
Figure 5: Courtesy of Carolyn Majcher, OD, FAAO.
Fundus autofluorescence (FAF)
With the use of fundus autofluorescence (FAF), it is possible to see areas where GA may develop, which appear as hyperfluorescent. Meanwhile, the GA lesions appear as dark, circular areas with well-demarcated borders.
FAF has the ability to highlight areas of subclinical GA that could prove difficult to detect employing color fundus photography or ophthalmoscopy alone.
GA management and patient education
The first step in ensuring a patient becomes an active participant in their care is to provide ample education. With GA, an integral part of this education is to emphasize the goal of treatment. Though treatment cannot reverse the structural damage or impaired sight, it can significantly slow the rate of vision loss over time.
With this patient, the extrafoveal nature of the lesions, OCT biomarkers, and documented progression, coupled with the current state of vision, make him an ideal candidate to be referred for either pegcetacoplan or avacincaptad pegol injections.
Therefore, education would involve informing him that he is an appropriate candidate for a complement inhibitor therapy delivered through intravitreal injections at 1- to 2-month intervals. However, it is prudent to make him fully aware that this therapy is chronic and requires continuity of care to receive the maximum benefit.
Subsequently, it is imperative to review the safety profile of the currently available therapies, including potential adverse events with patients.5 Armed with this knowledge, the individual can be equipped to share in the decision-making process on whether they wish to pursue treatment.
Conclusion
The case presented in this article provides a clear window into how advancements in both imaging and pharmacology have altered the future course of GA treatment.
Multimodal imaging studies can enable ECPs to proactively detect and predict the course of the disease, while complement inhibitor intravitreal therapies offer a level of hope to patients to possibly maintain vision for a longer period of time.


